Diagnostics of Subclinical Optic Nerve Damage by Optical Coherence Tomography in Multiple Sclerosis Patients
Abstract
Evaluation of the afferent visual system may give insight into ongoing neuro-degenerative processes in multiple sclerosis (MS) patients. The aim of our study is to assess the utility of optical coherence tomography (OCT) for sub-clinically damaged optic nerve diagnostics and to characterise retinal nerve fibre layer (RNFL) changes in MS patients without previous optic neuritis.
The cross-sectional study included 43 relapsing/remitting MS patients (86 eyes) without visual acuity changes and historical evidence of optic nerve inflammation. Measures included clinical characteristics and the RNFL measures in six standard sectors (temporal (RNFL T), temporal upper (RNFL TS), temporal lower (RNFL TI), nasal (RNFLT N), nasal upper (RNFLT NS), nasal lower (RNFLT NI).
In the eyes of MS patients, there was found a significantly decreased average RNFL thickness in RNFL T, RNFL TS, RNFL TI, RNFLT N and RNFLT NS sectors compared to controls (p < 0.05). However, this difference was not significant in RNFL NI sector (p = 0.97). Basing on the ROC curve analysis, it was detected that the major difference was observed in the RNFL T and RNFL TI sectors (as follows: AUC = 0.72, AUC = 0.75, p < 0.05). RNFL reduction in RNFL T sector was identified in 33.72% of MS patients (n = 29).
Significant thinning of RNFL obtained by OCT was found in one third of MS patients without previous demyelinating event in optic nerves. The most pronounced changes were observed in temporal sector without significant difference in nasal sector. Presumably, attention for further neurodegenerative process analysis should be focused on the temporal sector monitoring in the asymptomatic MS patients group.
Introduction
Multiple sclerosis (MS) is a chronic inflammatory and autoimmune central nervous system disorder that is mainly diagnosed clinically, basing on the evidence about lesion dissemination in space and time [Polman, 2011]. An episode of acute optic neuritis (ON) is observed in about 50% of MS patients during the course of disease [Frohman, 2005; Balcer, 2006]. Damage of the vision pathways has increased an interest among MS specialists, as it may be an ideal model for neurodegenerative process monitoring [Sakai, 2011]. Optical coherence tomography (OCT) creates images from retina, the only place, where direct axonal tissue layer examination is possible regardless of the myelin sheath thickness [Jindahra, 2011]. It is repeatedly shown that the retinal nerve fibre layer (RNFL) damage, diagnosed with OCT method may be observed after acute ON episode and even in the eyes without a history of ON. Quite often in these studies, RNFL assessment of the fellow, ON intact eye in patients with a history of ON was carried out [Parisi, 1999; Trip, 2005; Fisher, 2006; Garcia-Martin, 2011].
Aim
The aim of our study is to assess the utility of OCT for sub-clinically damaged optic nerve diagnostics and to characterise RNFL changes in MS patients without ON history.
Material and methods
The cross-sectional study included 43 relapsing/remitting multiple sclerosis patients with Snellen acuities of 20/20 in both eyes and without ON symptoms or clinical signs in history.
Patients were recruited from the Multiple Sclerosis Centre at Pauls Stradiņš Clinical University Hospital. Patients suffering from other neurological diseases but MS, ophthalmological or systemic ones, which could affect the afferent visual system, were not included in the study. Clinically definite MS diagnosis was established by an experienced neurologist based on McDonald’s criteria. An experienced ophthalmologist performed a complete ophthalmologic examination: determination of visual acuity, measurement of ocular tension, bio-microscopic examination of the anterior pole and visual field detection.
The OCT (Heidelberg Engineering SPECTRALIS) measured RNFL thickness in six standard sectors (temporal (RNFL T), temporal upper (RNFL TS), temporal lower (RNFL TI), nasal (RNFLT N), nasal upper (RNFLT NS), nasal lower (RNFLT NI)) for all subjects, using Tru Track Active Eye Tracking technology. All scans were performed by the same ophthalmologist. Poor quality scans were rejected. Presence of the defect was determined based on the machine normative database; a red coloured quadrant was classified as abnormal.
Descriptive statistics were performed according to data type. The statistical difference of quantitative variables for both groups was analysed using the Student’s t test. The level of significance for all statistical tests was set at p < 0.05. The receiver operating characteristic (ROC) curve and the area beneath it were analysed. We used MedCalc 12.0 software to estimate the statistical significance of the differences between the ROC curves areas.
Results
In the study, 86 eyes of MS patients were analysed, mean age (m = 39.58, SD = 10.81), the minimum age of patients was 17 years, the maximum age – 65 years, modal, or the most common age was 36 years. The control group consisted of 16 individuals (32 eyes). Basing on the independent t test, it was concluded that patients of the MS group (m = 39.58, SD = 10.81) were statistically significantly (p < 0.001) by 6.58 years older than the control group (m = 33.00; SD = 9.47).
In the eyes of MS patients without a history of ON, significant decrease of average RNFL thickness in RNFL T, RNFL TS, RNFL TI, RNFLT N and RNFLT NS sectors was found, compared to controls (p < 0.05). However, in RNFL NI sector RNFL thickness did not differ statistically significantly (p = 0.97) between the two groups. Analysis of the mean RNFL in different eye sectors in MS patients and control group has been represented in the Figure 1.
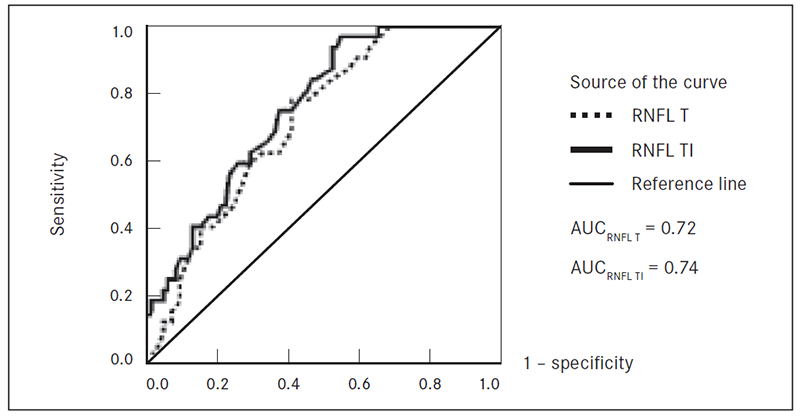
Basing on the ROC curve analysis, making the assessment of differences in the characteristics of MS patients and control group, it was found that the major difference is observed in the RNFL T and RNFL TI sectors (as follows: AUC = 0.72, AUC = 0.75, p < 0.05) (Fig. 2). Overall, RNFL reduction in RNFL T sector was seen in 33.72% of MS patients (n = 29).
Figure 1. The mean RNFL thickness in different sectors in MS patients without ON and control group
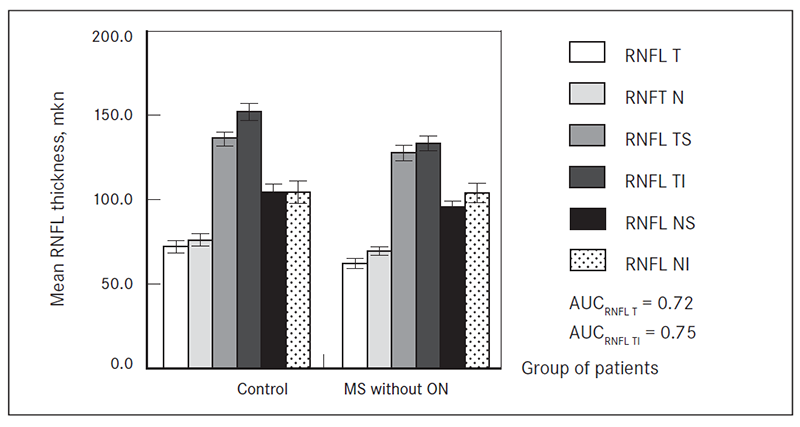
Figure 2. Assessment of RNF T and RNFL TI measurement suitability using ROC curves
Discussion
The course of MS disease is very unpredictable and varies from patient to patient. There is an increasing necessity for biological marker that could assess ongoing neuro-degeneration. OCT is highly reproducible, objective, non-invasive and easy test for axonal tissue damage evaluation. Similar to previously published studies [Parisi, 1999; Trip, 2005; Fisher, 2006; Garcia-Martin, 2011], our results show that eyes of MS patients without a previous ON episode have considerable abnormalities in OCT studies. Our findings suggest that the most marked changes affect the temporal RNFL sectors, both in the upper and lower quadrant, but practically no RNFL changes are observed at the lower nasal sector.
In the cases after an ON episode, axonal damage appears to be secondary to demyelination [Sakai, 2011]. However, the above-mentioned findings suggest about other than ON axonal damage mechanism that continues progressively and sub-clinically in the MS patient’s afferent visual system independently from the direct demyelinating process. These results support the need to apply OCT test to MS patients even without a history of ON in order to obtain information about axonal tissue damage. Relying on the data we have obtained, about 30% of asymptomatic MS patients have already had significant axonal tissue involvement before ON episode. It is likely that the damage mostly related to retrograde axonal degeneration, probably due to MS lesions in the radiatio optica area [Jindahra, 2009], but this mechanism is not fully understood yet and needs further evaluation.
Conclusion
Significant thinning of RNFL obtained by means of OCT was found in one third of MS patients without previous demyelinating event in optic nerves. The most pronounced changes were observed in the temporal sector without significant difference in the nasal sector. Targeted analysis by OCT in temporal sector in asymptomatic MS patients group in the future could provide additional information about neurodegenerative processes in different clinical and therapeutic situations.
References
- Balcer L. J. Clinical practice. Optic neuritis // N Engl J Med, 2006; 354 (12): 1273–1280.
- Fisher J. B., Jacobs D. A., Markowitz C. E., et al. Relation of visual function to retinal nerve fiber layer thickness in multiple sclerosis // Ophthalmology, 2006; 13 (2): 324–332.
- Frohman E. M., Frohman T. C., McColl R., Zee D., S. et al. The neuro-ophthalmology of multiple sclerosis // Lancet Neurol, 2005; 4 (2): 111–121.
- Ara J. R., Garcia-Martin E., Pueyo V., et al. Effect of optic neuritis on progressive axonal damage in multiple sclerosis patients // Mult Scler, 2011; 17 (7): 830–837.
- Jindahra P., Hedges T. R., Mendoza-Santiesteban C. E., Plant G. T. Optical coherence tomography of the retina: applications in neurology // Curr Opin Neurol, 2010; 23 (1): 16–23.
- Jindahra P., Petrie A., Plant G. T. Retrograde trans-synaptic retinal ganglion cell loss identified by optical coherence tomography // Brain, 2009; 132 (Pt 3): 628–634.
- Manni G., Parisi V., Spadaro M., et al. Correlation between morphological and functional retinal impairment in multiple sclerosis patients. // Invest Ophthalmol Vis Sci, 1999; 40 (11): 2520–2527.
- Banwell B., Polman C. H., Reingold S. C., et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria // Annals of Neurology, 2011; 69 (2): 292–302.
- Feller D. J., Galetta K. M., Sakai R. E., et al. Vision in multiple sclerosis: The story, structure-function correlations, and models for neuroprotection // J Neuroophthalmol, 2011; 31 (4): 362–373.
- Jones S. J., Schlottmann P. G., Trip S. A., et al. Retinal nerve fiber layer axonal loss and visual dysfunction in optic neuritis // Ann Neurol, 2005; 58 (3): 383–391.



