Safety and Efficacy of Narcotrend Controlled Sedation with Dexmedetomidine vs. Propofol during Elective Colonoscopy
Abstract
The aim of the study was to evaluate safety and efficacy of sedation with dexmedetomidine vs. propofol during elective colonoscopy.
72 patients ASA I–III undergoing colonoscopy, included in a prospective study, were randomised into two groups of 36: dexmedetomidine (group D) (1 μg/kg/10 min, followed by 0.2–0.6 μg/kg/h) or propofol (group P) (TCI 2–6 μg/ml).
Depth of sedation was assessed by Narcotrend monitoring and sedation scales. Rescue analgesics (fentanyl i/v 0.1 mg) were used by procedure needs.
Safety was determined by hemodynamic (heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP)) and respiratory parameters, and patients discharge time from hospital. Efficacy was determined by sedation score and satisfaction of patients and endoscopists.
Demographic characteristics of patients were similar in both groups.
In group D, after 10 minutes mean HR decreased from 75.0 ± 11.9 to 60.1 ± 8.7 ×/min (−19.0 %) (p < 0.001), atropine was required in seven (19.4 %) patients, mean SBP – from 142.4 ± 22.9 to 121.1 ± 20.1 mm Hg (−15.0 %) (p < 0.001), mean DBP – from 70.6 ± 11.9 to 63.9 ± 11.6 mm Hg (−9.5 %) (p < 0.001), six (16.7 %) patients had hypotension treated with i/v fluid.
In group P, after 10 minutes mean HR decreased from 80.2 ± 13.6 to 68.7 ± 12.1 ×/min (−14.3 %) (p < 0.001), atropine was required in one (2.8 %) patient, mean SBP – from 142.2 ± 30.4 to 110.7 ± 23.7 mm Hg (−22.1 %) (p < 0.001), mean DBP – from 70.6 ± 12.9 to 60.1 ± 12.4 mm Hg (−14.9 %) (p < 0.001), three (8.3 %) patients had hypotension treated with i/v fluid.
All patients in both g roups had spontaneous breathing during a ll procedure. In group D, six (16.7 %) patients required O supply vs. 25 (69.4 %) in group P. Jaw thrust was required only in 10 cases in group P.
Although there was difference between the groups’ mean NI after induction (group D: 82.2 ± 10.4, group P: 71.8 ± 19.3, p < 0.001), patients in both groups fell asleep, but after insertion of colonoscope in group D, NI was higher (group D: 97.0 ± 1.9, group P: 69.4 ± 17.6, p < 0.001), to advance the procedure rescue analgesics were required to all patients in group D and only one patient in group P.
More frequently patients in group P than patients in group D were satisfied or highly satisfied with the received sedation (94.5 % vs. 44.4 %, p < 0.001).
Dexmedetomidine use at a loading dose of 1.0 μg/kg/10 min caused dissatisfaction in endoscopists.
Sedation with dexmedetomidine more frequently cause bradycardia required for atropine (20 % vs. 3 %) and longer discharge time, but sedation with propofol more frequently cause adequate spontaneous breathing depression.
Sedation with dexmedetomidine cause less satisfaction of both patients and endoscopists.
Introduction
Nowadays colonoscopy is the standard procedure for diagnosis, screening, treatment and follow up for many colorectal diseases. Although some patients can tolerate colonoscopy without any sedation and analgesics requirements, it is a distressful procedure for most patients (Techanivate et al., 2012). Conscious sedation is a common strategy for improving patient comfort during this procedure that is typically not well tolerated (Nishizawa et al., 2017). Patients should be kept at a level where they can respond to verbal commands and should respond purposefully when stimulated. Spontaneous ventilation is adequate, cardiovascular function is usually maintained (Amornyotin et al., 2014).
Sedation for colonoscopy using intravenous propofol has become standard in many countries (Riphaus et al., 2017) because of its rapid onset and offset of action. The most important disadvantage of propofol is the risk of rapidly induced deep sedation, with possibility to respiratory and cardiovascular depression (Eberl et al., 2016).
Dexmedetomidine is quite a new short-acting selective α2-agonist which recently has entered the medicine of Latvia with sedative, anxiolytic and analgesic properties and appears to have no clinically important adverse effects on respiration (Eberl et al., 2013). However, although dexmedetomidine seems to be an alternative option for sedation during colonoscopy procedures the sympatholysis it induces can cause hypotension and bradycardia (Riphaus et al., 2017).
Aim
The aim of the study was to evaluate safety and efficacy of sedation with dexmedetomidine vs. sedation with propofol during elective colonoscopy procedure.
Material and Methods
This prospective, randomised, single-blind study was conducted with a population of patients undergoing ambulatory elective colonoscopy in Riga East Clinical University Hospital “Gaiļezers”, Latvia. The study was approved by the Ethical Committee of Rīga Stradiņš University (Riga, Latvia), and written, informed consent was obtained from all of the participants.
Eligible patients for participation in this clinical study were those scheduled for elective colonoscopy, aged above 18 years and American Society of Anaesthesiologists physical status (ASA) I–III, who have given the written informed consent.
The exclusion criteria were as follows: non-invasive systolic blood pressure < 90 mm Hg, heart rate < 60 beats per minute and / or related brady-dysrhythmias (advanced heart block), impaired liver function, impaired renal function, know allergic or adverse reaction to dexmedetomidine or propofol (soy bean, egg), pregnancy, psychiatric or emotional disorder, chronic use of or addiction to opiates, sedatives or antidepressants.
A total of 72 adult patients were randomly allocated into two groups of 36 to receive either dexmedetomidine or propofol sedation in a 1 : 1 ratio. The study flow chart is shown in Figure 1.
Figure 1. Study flow chart
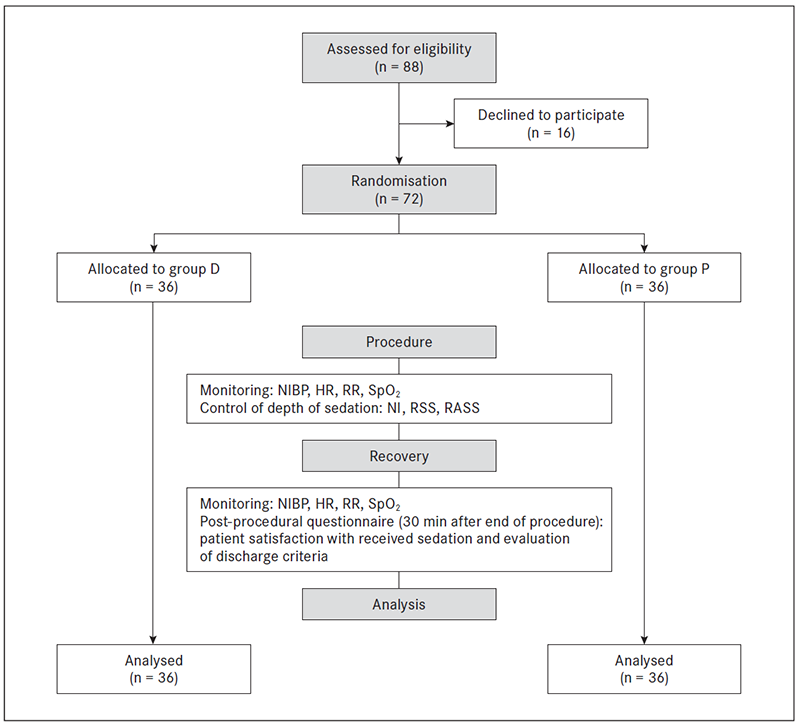
D – dexmedetomidine; HR – heart rate; n – number of patients; NI – Narcotrend index; NIBP – non-invasive blood pressure; P – propofol; RASS – Richmond Agitation Sedation Score; RR – respiratory rate; RSS – Ramsey Sedation Score; SpO2 – peripheral oxygen saturation.
Sedative Intervention
Patients were blinded to the sedation regimen they were supposed to get. Sedation within both groups was performed by an anaesthesiologist and anaesthesia nurse who were not blinded to the used form of sedation. Endoscopist and endoscopic nurse were also not blinded.
No premedication was provided in all cases.
In dexmedetomidine (D) group, patients received a loading dose of intravenous dexmedetomidine (Dexdor: Orion Corporation, Finland) 1 μg/kg over 10 minutes. After this loading bolus, the procedure was started and dexmedetomidine continued throughout the procedure till ileocecal valve was reached within the range of 0.2–0.6 μg/kg/h titrated to a targeted level of sedation.
In propofol (P) group, patients received sedation with propofol (Propofol 1 % MCT Fresenius, Germany) using a propofol Target Controlled Infusion (TCI) system Schnider Effect Site pharmacokinetic model, starting with a targeted effect site concentration of 2 μg/ml titrated to a targeted level of sedation continued till ileocecal valve was reached. Rescue analgesics (0.1 mg intravenous fentanyl) were given in response to pain.
All patients had continuous EEG recording in an attempt to assess depth of sedation using Narcotrend monitoring. Patients were assessed for the level of sedation before sedatives were given (baseline), after induction dose before the colonoscopy started, when colonoscopy started (insertion of colonoscope), after first 5 and 10 minutes of colonoscopy, after the end of colonoscopy (withdrawal of colonoscope) and during recovery in a procedure room. Narcotrend is an electroencephalogram (EEG) monitor designed to measure the depth of sedation. Narcotrend algorithm is based on pattern recognition of the raw EEG and classifies the EEG traces into different stages from A (awake) to F (increasing burst suppression down to electrical silence) referring to a range of Narcotrend index from 100 (awake) to 0 (electrical silence) (see Table 1) (Kreuer et al., 2004; Kreuer & Wilhelm, 2006).
Level of sedation was measured also by Ramsey Sedation Scale (RSS) (see Table 2) and Richmond Agitation Sedation Scale (RASS) (see Table 3) (Sessler, Grap & Ramsey, 2008) five minutes after insertion of colonoscope.
Table 1. Narcotrend stages and the respective Narcotrend index ranges
| Clinical condition | Narcotrend stage | Narcotrend index |
|---|---|---|
| Awake | A | 95–100 |
| Sedated | B | 80–94 |
| Light anaesthesia | C | 65–79 |
| General anaesthesia | D | 37–64 |
| General anaesthesia with deep hypnosis | E | 13–36 |
| General anaesthesia with increasing burst suppression | F | 0–12 |
Table 2. Ramsey Sedation Scale
| Score | Definition |
|---|---|
| 1 | Anxious and agitated or restless or both |
| 2 | Cooperative, oriented and tranquil |
| 3 | Responds to commands only |
| 4 | Brisk response to a light glabellar tap or loud auditory stimulus |
| 5 | Sluggish response to a light glabellar tap or loud auditory stimulus |
| 6 | No response to a light glabellar tap or loud auditory stimulus |
Table 3. Richmond Agitation Sedation Scale
| Score | Term | Description |
|---|---|---|
| +4 | Combative | Overtly combative or violent, immediate danger to staff |
| +3 | Very agitated | Pulls on or removes tube(s) or catheter(s) or exhibits aggressive behaviour towards staff |
| +2 | Agitated | Frequent non-purposeful movement or patient-ventilator dyssynchrony |
| +1 | Restless | Anxious or apprehensive but movements non-aggressive or vigorous |
| 0 | Alert and calm | |
| -1 | Drowsy | Not fully alert, but has sustained (> 10 seconds) awakening, with eye contact to voice |
| -2 | Light sedation | Briefly (< 10 seconds) awakens with eye contact to voice |
| -3 | Moderate sedation | Any movement (but no eye contact) to voice |
| -4 | Deep sedation | No response to voice, but any movement to physical stimulation |
| -5 | Unarousable | No response to voice or physical stimulation |
Colonoscopy Procedure and Monitoring
Colonoscopies were performed by three experienced endoscopists using a video colonoscope.
The following parameters were measured continuously and recorded every five minutes: heart rate (HR), non-invasive systolic (SBP) and diastolic (DBP) blood pressure, respiratory rate (RR), peripheral oxygen saturation (SpO2).
Total procedure time, all drugs, drug amounts and time of administration, time from the end of the procedure until discharge time, any respiratory and cardiovascular event or other complications and side effects (nausea, vomiting, dizziness) and all actions visibly taken to prevent or treat these problems, such as supply of oxygen, apply of jaw thrust, bag-mask ventilation or use of any airway device, were also recorded.
If the event of bradycardia (HR < 50 bpm) occurred, 0.5 mg of atropine was administrated. In case of hypotension (SBP < 90 mm Hg), normal saline solution was administrated intravenously. If SpO2 decreased to 94 % or less, oxygen was delivered by facemask. If oxygen supply did not help to increase SpO2, a jaw thrust manoeuver was applied.
Outcome Assessment
The primary outcome was safety of sedation, determined by hemodynamic and respiratory parameters, need for oxygen supply and a jaw thrust manoeuver application, need for bag-mask ventilation and / or use of any airway device and patients discharge time from hospital.
A secondary outcome was efficacy of sedation, classified by sedation score and satisfaction levels of patients and endoscopists.
In recovery room 30 minutes after the end of procedure, patients were asked to rate their satisfaction or dissatisfaction with the received sedation ranging from 1 (very dissatisfied) to 5 (highly satisfied), and discharge criteria was assessed.
Discharge criteria require that a patient is awake and alert with stable vital signs, is able to ambulate without assistance and is free of side effects of the drugs employed during the procedure.
Satisfaction of endoscopists with both sedation forms was assessed in the end of clinical study period.
Statistical Methods
Data statistical analysis was performed using Microsoft Excel 2016 and SPSS 22.0 (Statistical Package for Social Sciences). All data were checked for normal distribution using Kolmogorov-Smirnov and Shapiro-Wilk tests. For normally distributed data Student’s T test, Chi-Square test was used. Non-normally distributed data were compared using Mann-Whitney test. A p value of less than 0.05 was considered significant.
Results
In total, 72 patients were included into the study; 36 patients received propofol (group P) and another 36 received dexmedetomidine (group D). All patients successfully completed colonoscopy procedure.
There was no significant difference between the groups regarding demographic characteristics, ASA and mean duration of colonoscopy (see Table 4).
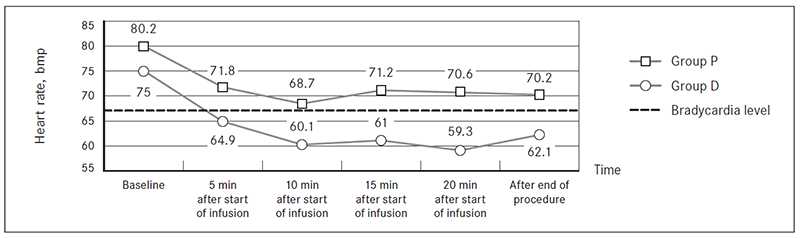
Mean HR 10 minutes after the start of infusion in group D decreased f rom 75.0 ± 11.9 bpm to 60.1 ± 8.7 bpm (−19.9 %; p < 0.0001) (see Table 5).
Mean HR 10 minutes after the start of infusion in group P decreased f rom 80.2 ± 13.6 bpm to 68.9 ± 12.1 bpm (−14.1 %; p < 0.0001) (see Table 5).
In group D, mean HR almost approached bradycardia level (60 bmp) 10, 15, 20 minutes after the start of infusion, not observed in group P (Figure 2).
Mean systolic blood pressure 10 minutes after the start of infusion in group D decreased from 142.4 ± 23.0 mm Hg to 121.1 ± 20.1 mm Hg (−15.0 %; p < 0.0001), mean diastolic blood pressure decreased from 70.6 ± 11.9 mm Hg to 63.9 ± 11.6 mm Hg (−9.5 %; p < 0.0001) (see Table 6).
Table 4. Patients’ characteristics and procedure data
| Parameters | Group D | Group P | p value |
|---|---|---|---|
| Female, n (%) | 19 (52.8) | 25 (69.4) | 0.648 |
| Male, n (%) | 17 (47.2) | 11 (30.6) | 0.618 |
| Mean age, years | 57.6 ± 16.5 | 63.0 ± 15.0 | 0.140 |
| Mean body mass, kg | 78.4 ± 13.3 | 78.5 ± 13.0 | 0.978 |
| Mean body mass index, kg/m2 | 26.3 ± 2.8 | 28.0 ± 4.8 | 0.099 |
| ASA I, n (%) | 18 (50.0) | 12 (33.3) | 0.324 |
| ASA II, n (%) | 15 (41.7) | 18 (50.0) | |
| ASA III, n (%) | 3 (8.30) | 6 (16.7) | |
| Mean duration of colonoscopy, min | 15.6 ± 5.2 | 15.6 ± 5.6 | 0.778 |
ASA – American Society of Anaesthesiologists’ physical status; D – dexmedetomidine; P – propofol.
Table 5. Mean heart rate during sedation in both groups (beats per minute, SM ± SD)
| Time | Group D | Group P | p value |
|---|---|---|---|
| Baseline | 75.0 ± 11.9 | 80.2 ± 13.6 | 0.070 |
| 5 min after start of infusion | 64.8 ± 9.7 | 71.8 ± 10.7 | 0.003 |
| 10 min after start of infusion | 60.1 ± 8.7 | 68.7 ± 12.1 | 0.002 |
| 15 min after start of infusion | 61.0 ± 10.3 | 71.2 ± 11.2 | < 0.001 |
| 20 min after start of infusion | 59.3 ± 7.9 | 70.6 ± 12.1 | 0.001 |
| After the end of the procedure | 62.1 ± 8.2 | 70.2 ± 10.4 | < 0.001 |
D – dexmedetomidine; P – propofol; SM – statistic mean; SD – standard deviation.
Figure 2. Changes in mean heart rate during sedation in both groups
Mean systolic blood pressure 10 minutes after the start of infusion in group P decreased from 142.2 ± 30.4 mm Hg to 110.7 ± 23.7 mm Hg (−22.2 %; p < 0.0001) mean diastolic blood pressure decreased from 70.6 ± 12.9 mm Hg to 60.1 ± 12.4 mm Hg (−14.9 %; p < 0.0001) (see Table 6).
Both dexmedetomidine and propofol induced decreases in systolic and diastolic blood pressure after the start of infusion. In group P, significantly larger systolic blood pressure decrease was observed at the 5th (p = 0.002) and 10th (p = 0.022) minute and after the end of the procedure (p = 0.010), and diastolic blood pressure decreased at the 5th (p < 0.0001) minute and after the end of the procedure (p = 0.002) as compared with group D (see Table 6).
Negligible respiratory rate variations were observed in both study groups.
All patients in both groups had spontaneous breathing during the entire procedure, no patient required bag-mask ventilation or use of any airway device (see Table 7).
Table 6. Mean systolic and diastolic blood pressure (SM ± SD) during sedation in both groups (mm Hg)
| Time | Group D | Group P | p value SBP | p value DBP | ||
|---|---|---|---|---|---|---|
| SBP | DBP | SBP | DBP | |||
| Baseline | 142.4 ± 23.0 | 70.6 ± 11.9 | 142.2 ± 30.4 | 70.6 ± 12.9 | 0.972 | 0.992 |
| 5 min after start of infusion | 129.8 ± 20.3 | 66.8 ± 10.8 | 111.4 ± 22.0 | 57.0 ± 13.3 | 0.002 | < 0.001 |
| 10 min after start of infusion | 121.1 ± 20.1 | 63.9 ± 11.6 | 110.7 ± 23.7 | 60.1 ± 12.4 | 0.022 | 0.200 |
| 15 min after start of infusion | 116.3 ± 19.9 | 61.7 ± 11.9 | 109.8 ± 25.0 | 61.0 ± 15.5 | 0.067 | 0.838 |
| 20 min after start of infusion | 113.9 ± 22.1 | 62.2 ± 12.6 | 112.0 ± 28.7 | 61.3 ± 14.9 | 0.502 | 0.855 |
| After the end of the procedure | 116.6 ± 18.3 | 65.0 ± 9.4 | 105.2 ± 15.9 | 57.3 ± 10.9 | 0.010 | 0.002 |
D – dexmedetomidine; DBP – diastolic blood pressure; P – propofol; SBP – systolic blood pressure; SM – statistic mean; SD – standard deviation.
Table 7. Respiratory and cardiovascular events and actions taken to treat these problems
| Respiratory and cardiovascular events and actions | Number of patients, n (%) | p value | |
|---|---|---|---|
| Group D | Group P | ||
| Need for bag-mask ventilation and / or use of any airway device | 0 | 0 | – |
| Need for oxygen supply | 6 (16.7) | 25 (69.4) | < 0.001 |
| Need for a jaw thrust manoeuver apply | 0 | 10 (27.8) | < 0.001 |
| Bradycardia required for atropine | 7 (19.4) | 1 (2.8) | 0.028 |
| Hypotension required for fluid infusion | 6 (16.7) | 3 (8.3) | 0.239 |
D – dexmedetomidine; P – propofol.
To maintain SpO2 ≥ 94 %, in group D six (16.7 %) patients and in group P 25 (69.4 %) patients required oxygen supply. A jaw thrust manoeuver had to be applied in 10 of the cases (27.8 %) in group P. This was not required in group D. Patients receiving sedation with dexmedetomidine required oxygen supply (p < 0.0001) and achievement of correct airway (p < 0.0001) less frequently than patients receiving sedation with propofol (see Table 7).
There were seven (19.4 %) patients in group D and one (2.8 %) patient in group P who developed bradycardia and were given atropine. Three patients in group D received the second dose of atropine because bradycardia repeated the second time after the first dose of atropine was given. In group D, bradycardia in range from 44 bpm to 47 bpm developed in interval between the 4th and the 17th minute of infusion. One patient receiving dexmedetomidine had the third episode of bradycardia (HR 43 bpm) three hours after the end of the procedure, atropine was given the third time, and after one hour the patient was discharged from hospital with HR 61 bpm. Patients receiving sedation with dexmedetomidine had more frequent cases of bradycardia required for atropine (p = 0.028) than patients receiving sedation with propofol (see Table 7).
There were six (16.7 %) patients in group D and three (8.3 %) patients in group P who developed hypotension and normal saline solution was administrated intravenously. In all patients SBP was increased to normal SBP range after fluid infusion. The incidence of hypotension were insignificantly different between the study groups (p = 0.239) (see Table 7).
Dizziness (two patients) and nausea (one patient) were observed after the procedure only in group D.
Most patients (77.8 %) in group D and almost all patients (94.4 %) in group P were discharged from hospital 30 minutes after the end of procedure (Figure 3). Mean time to home readiness was insignificantly longer in group D (49.5 min and 32.5 min in groups D and P, respectively (p = 0.336).
Discharge was delayed in group D patients because of the following factors: prolonged drowsiness (six cases), dizziness (two cases), nausea (one case) and bradycardia (one case).
Mean NI in group D after induction of sedation decreased from 98.8 ± 0.6 to 82.2 ± 10.4 (−16.7 %; p < 0.0001), in group P – from 98.4 ± 1.0 to 71.8 ± 19.3 (−27.0 %; p < 0.0001) (see Table 8). Although there was a significant difference between the groups’ mean NI after induction (p < 0.0001), patients in both groups after induction fell asleep. Insertion of colonoscope woke up patients in group D. Mean NI was significantly higher and depth of sedation was significantly lower during all colonoscopy procedure in patients receiving sedation with dexmedetomidine. When patients in group D remain unstimulated – after withdrawal of colonoscope, they returned to sedated state (NI 87.3 ± 5.5).
Supplemental fentanyl was required in all 36 (100.0 %) patients receiving dexmedetomidine and only in one (2.8 %) patient receiving propofol to achieve a satisfactory level of sedation to proceed with the procedure (p < 0.0001).
When the depth of sedation between the groups was compared using the RSS (see Table 9) and RASS (see Table 10), the scores of group D, at the 5th minute after colonoscopy was started, were significantly higher than those of group P.
Although NI monitoring during all colonoscopy procedure in group D showed that patients were awake (NI 94.6–97.0), most patients were cooperative, oriented and tranquil, evaluated by RSS, or alert and calm, evaluated by RASS.
Figure 3. Discharge time from hospital after the end of the procedure
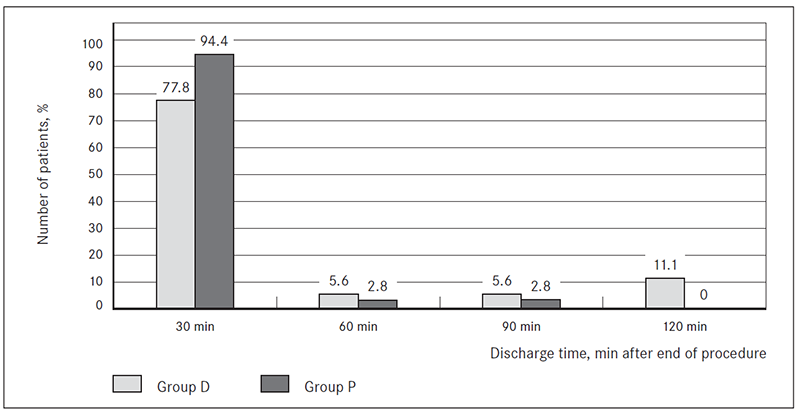
Table 8. Mean Narcotrend index (SM ± SD) during sedation in both groups
| Time | Group D | Group P | p value |
|---|---|---|---|
| Baseline | 98.8 ± 0.6 | 98.4 ± 1.0 | 0.169 |
| After induction (before insertion of colonoscope) | 82.2 ± 10.4 | 71.8 ± 19.3 | < 0.001 |
| Insertion of colonoscope | 97.0 ± 1.9 | 69.4 ± 17.6 | < 0.001 |
| 5 min after insertion | 95.3 ± 2.9 | 58.8 ± 19.9 | < 0.001 |
| 10 min after insertion | 94.6 ± 3.3 | 65.7 ± 19.7 | < 0.001 |
| Withdrawal of colonoscope | 87.3 ± 5.5 | 81.6 ± 14.6 | < 0.001 |
| During recovery in procedure room | 96.53 ± 1.58 | 97.76 ± 1.06 | 0.001 |
D – dexmedetomidine; P – propofol; SM – statistic mean; SD – standard deviation.
Table 9. Measuring depth of sedation using Ramsey Sedation Score in both groups
| Score | Number of patients, n (%) | p value | |
|---|---|---|---|
| Group D | Group P | ||
| 1 | 5 (13.9) | 0 | 0.037 |
| 2 | 23 (63.9) | 0 | < 0.001 |
| 3 | 5 (13.9) | 2 (5.6) | 0.238 |
| 4 | 3 (8.3) | 14 (38.9) | 0.009 |
| 5 | 0 | 20 (55.6) | < 0.001 |
| 6 | 0 | 0 | – |
D – dexmedetomidine; P – propofol.
Table 10. Measuring depth of sedation using Richmond Agitation Sedation Scale in both groups
| Score | Number of patients, n (%) | p value | |
|---|---|---|---|
| Group D | Group P | ||
| +4 | 0 | 0 | – |
| +3 | 0 | 0 | – |
| +2 | 0 | 0 | – |
| +1 | 5 (13.9) | 0 | 0.037 |
| 0 | 22 (61.1) | 0 | < 0.001 |
| -1 | 2 (5.6) | 0 | 0.337 |
| -2 | 5 (13.9) | 3 (8.3) | 0.338 |
| -3 | 2 (5.6) | 12 (33.3) | 0.024 |
| -4 | 0 | 21 (58.3) | < 0.001 |
| -5 | 0 | 0 | – |
D – dexmedetomidine; P – propofol.
From analysis of post-procedure questionnaires, satisfaction scores of sedation and remembrance of the procedure among patients was significantly different between the groups. Only 44.4 % of all the patients in group D were satisfied or highly satisfied with the received form of sedation, and 94.5 % of all the patients in group P (p < 0.001). 33 (91.7 %) patients in group D and five (13.9 %) patients in group P recalled mild to moderate pain or discomfort during the colonoscopy procedure (p < 0.001).
Dexmedetomidine use at a loading dose of 1.0 μg/kg over 10 minutes, which resulted in a delay of the beginning of colonoscopy procedure, caused dissatisfaction of all three endoscopists, who performed all procedures.
Discussion
Sedation has always been a critical component of performing colonoscopy procedures which is an uncomfortable and stressful procedure for most patients. The aim of sedation for these procedures is to increase a patient’s comfort, improve endoscopic performance and increase patient and endoscopist satisfaction (Amornyotin et al., 2014). Over the past 15 years, propofol has become the drug of choice for sedation due to its favourable pharmaceutical properties and outstanding safety profile (Lewis & Cohen, 2013); however, propofol is associated with respiratory depression and airway obstruction (Amornyotin et al., 2014). There are many publications of propofol use for sedation during colonoscopies, even the effect of sex aspects were investigated when propofol is used as sedation for gastrointestinal endoscopy (Riphaus et al., 2017). The α2-receptor agonist dexmedetomidine has sedative and anxiolytic properties. At therapeutic doses, it is not associated with respiratory depression (Arain & Ebert, 2002). Because of these properties, it has been hypothesised that dexmedetomidine might prove useful outside the operating room for sedation for colonoscopies.
In literature, the described clinical study results of dexmedetomidine use for sedation during colonoscopy are still controversial.
Dere K. et al. (2010) comparing the effects of dexmedetomidine vs. midazolam during colonoscopy proved that dexmedetomidine provides more efficient hemodynamic stability, higher Ramsay sedation scale scores, higher satisfaction scores and lower numerical pain rating scale scores in colonoscopies. According to their results, dexmedetomidine can be used safely as a sedoanalgesic agent in colonoscopies.
Sula H. et al. (2012) compared sedation during colonoscopy with the standard regimen of propofol vs. dexmedetomidine. They concluded that both regimens are suitable for safe sedation during colonoscopy procedure. The authors found that the use of propofol caused more desaturation, whereas dexmedetomidine caused more hypotension. The latter result is similar to the clinical study performed within the study described in this article. We also found that patients receiving sedation with dexmedetomidine required less frequent oxygen supply and jaw thrust manoeuver application, but the incidence of hypotension was higher compared to patients receiving sedation with propofol. The research data indicated that 50 % of cases in patients sedated with propofol Narcotrend system showed deeper sedation level than moderate sedation. This can explain why adequate spontaneous breathing depression was observed more frequently in propofol group.
Jalowiecki et al. (2005) used dexmedetomidine, meperidine with midazolam or fentanyl on demand in colonoscopy and observed 4/19 (21.1 %) cases of hypotension (mean arterial pressure 50 % of baseline) in dexmedetomidine group, four (21.1 %) cases of bradycardia required for atropine and nine cases of pain that required additional opioids. From the analysis of the obtained results, in dexmedetomidine group hypotension treated with intravenous fluid infusion was performed in six cases (16.7 %), bradycardia required for atropine was observed in 7/36 (19.4 %) patients.
Risk for developing bradycardia is also highlighted in instruction of drug manufacturer (European Commission). Due to the potential bradycardia, the dose of dexmedetomidine was not increased; thus, adequate level of sedation as observed in propofol group could not be achieved. Patients sedated with dexmedetomidine during colonoscopy procedure were awake according to Narcotrend index, cooperative, oriented and tranquil, according to Ramsey Sedation Scale, or alert and calm, according to Richmond Agitation Sedation Scale. As a result of lower depth of sedation rescue analgesics were required in all patients receiving sedation with dexmedetomidine.
Although there was no significant difference between the groups regarding the incidence of hypotension, it was observed more frequently in dexmedetomidine group.
Developing of hypotension can explained by sympatholysis induced by dexmedetomidine (Eberl et al., 2016) and patients hypovolemia that is caused by bowel preparation to procedure (Lewis & Cohen, 2013), or even the combination of both factors.
At the beginning of year 2017, first meta-analysis was published where Nishizawa T. et al. (2017) compare dexmedetomidine vs. propofol for gastrointestinal endoscopy. They conducted meta-analysis of data from six randomised controlled trials that compared dexmedetomidine with propofol and concluded that, in gastrointestinal endoscopy, patient satisfaction level was higher in propofol administration, when compared to dexmedetomidine, but the risk of complications was similar. In the study perfomed within our research, dexmedetomidine sedation was also less satisfactory for patients than sedation with propofol, cardiovascular complications occurred more frequently in patients sedated with dexmedetomidine, but respiratory complications more frequently in patients sedated with propofol. Sedation with dexmedetomidine was less satisfactory for patients than sedation with propofol because the depth of sedation with dexmedetomidine was lower and did not provide an appropriate degree of memory loss or decreased awareness as provided by propofol sedation. Complicated administration regimen of dexmedetomidine resulted in less satisfaction than propofol among endoscopists, as well. Administration regimen and dosage of dexmedetomidine was in line with other studies and is in line with drug manufacturer recommendations and with the recommended maximum dosage approved by the Food and Drug Administration for procedural sedation.
The cost of dexmedetomidine should be taken into account, if practitioners are planning to use it in everyday practise. A two ml ampule of dexmedetomidine is still very expensive; its cost is significantly greater than an ampule of propofol, but when the patent of drug expires, generic drug will appear with a more available price.
Conclusions
- Comparing safety of sedation:
- sedation with dexmedetomidine more frequently causes bradycardia required for atropine (20 % vs. 3 %) and longer discharge time from hospital than sedation with propofol;
- sedation with propofol more frequently causes adequate spontaneous breathing depression required for oxygen supply and a jaw thrust manoeuver application than sedation with dexmedetomidine.
- Comparing efficacy of sedation:
- higher Narcotrend index and lower sedation scale scores of sedation with dexmedetomidine, and request for rescue analgesics to proceed with the procedure cause less satisfaction in patients;
- slow induction of dexmedetomidine sedation, which resulted in delay of the onset of colonoscopy procedure, causes dissatisfaction in endoscopists.
References
- Amornyotin, S. et al. 2014. Sedative and analgesic drugs for gastrointestinal endoscopic procedure [online]. Journal of Gastroenterology and Hepatology Research. 3 (7), 1133–1144. Available from: http://www.ghrnet.org/index.php/joghr/article/view/779 [viewed 10.05.2017].
- Amornyotin, S. 2013. Sedation and monitoring for gastrointestinal endoscopy. World Journal of Gastrointestinal Endoscopy. 5 (2), 47–55.
- Arain, S. A., Ebert, T. J. 2002. The efficacy, side effects, and recovery characteristics of dexmedetomidine vs. propofol when used for intraoperative sedation. Anaesthesia & Analgesia. 95, 461–466.
- Dere, K., Sucullu, I., Budak, E. T. et al. 2010. A comparison of dexmedetomidine vs. midazolam for sedation, pain and hemodynamic control, during colonoscopy under conscious sedation [online]. European Journal of Anaesthesiology. 27 (7), 648–652. Available from: https://www.ncbi.nlm.nih.gov/pubmed/20531094 [viewed 10.05.2017].
- Eberl, S., Preckel, B., Bergman, J. J. et al. 2016. Satisfaction and safety using dexmedetomidine or propofol sedation during endoscopic oesophageal procedures. European Journal of Anaesthesiology. 33, 631–637.
- Eberl, S., Preckel, B., Bergman, J. J., Hollmann, M. 2013. Safety and effectiveness using dexmedetomidine vs. propofol TCI sedation during oesophagus interventions: a randomized trial [online]. BMC Gastroenterology. 13 (1), 1. Available from: http://bmcgastroenterol.biomedcentral.com/articles/10.1186/1471-230X-13-176 [viewed 10.05.2017].
- European Commission, Public Health. Summary of product characteristics [online]. Brussels, Belgium. Available from: https://ec.europa.eu/health/documents/community-register/2013/20131218127652/anx_127652_en.pdf [viewed 18.05.2017].
- Jalowiecki, P., Rudner, R., Gonciarz, M. et al. 2005. Sole use of dexmedetomidine has limited utility for conscious sedation during outpatient colonoscopy. Anaesthesiology. 103 (2), 269–273.
- Kreuer, S., Bruhn, J., Larsen, R., et al. 2004. Comparability of NarcotrendTM index and bispectral index during propofol anaesthesia. British Journal of Anaesthesia. 93 (2), 235–240.
- Kreuer, S., Wilhelm, W. 2006. The Narcotrend monitor [online]. Best Practice and Research Clinical Anaesthesiology. 20 (1), 111–119. Available from: https://www.ncbi.nlm.nih.gov/pubmed/16634418 [viewed 10.05.2017].
- Lewis, J. R., Cohen, L. B. 2013. Update on colonoscopy preparation, premedication and sedation [online]. Expert Review of Gastroenterology & Hepatology. 7 (1), 77. Available from: http://www.medscape.com/viewarticle/778967_10 [viewed 10.05.2017].
- Nishizawa, T., Suzuki, H., Hoseo, N. et al. 2017. Dexmedetomidine vs. propofol for gastrointestinal endoscopy: A metaanalysis [online]. United European Gastroenterology Journal. 0 (0), 1–9. Available from: http://journals.sagepub.com/doi/10.1177/2050640616688140 [viewed 08.06.2017].
- Riphaus, A., Slottje, M., Bulla, J. et al. 2017. Women awaken faster than men after electroencephalogram-monitored propofol sedation for colonoscopy: A prospective observational study [online]. European Journal of Anaesthesiology. 6. Available from: http://journals.lww.com/ejanaesthesiology/Abstract/publishahead/Women_awaken_faster_than_men_after.98658.aspx [viewed 08.06.2017].
- Sessler, C., Grap, M., Ramsey, M. 2008. Evaluating and monitoring analgesia and sedation in the intensive care unit [online]. Critical Care. 12 (Suppl 3), S2. Available from: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2391268/ [viewed 18.05.2017].
- Sula, H., Domi, R., Ohri, I. et al. 2012. Propofol vs. dexmedetomidine for sedation in colonoscopy: a prospective, randomized study [online]. European Journal of Anaesthesiology. 6 (29), 32. Available from: http://journals.lww.com/ejanaesthesiology/Fulltext/2012/06001/Propofol_versus_dexmedetomidine_for_sedation_in.105.aspx [viewed 18.05.2017].
- Techanivate, A, Verawattaganon, T, Saiyuenyong, C, Areeruk, P. A. 2012. Comparison of dexmedetomidine vs. propofol on hypotension during colonoscopy under sedation [online]. Journal of Anaesthesia and Clinical Research. 10 (3), 257. Available from: https://www.omicsonline.org/a-comparison-of-dexmedetomidine-versus-propofol-on-hypotension-during-colonoscopy-under-sedation-2155-6148.1000257.php?aid=9444 [viewed 22.05.2017].



