Clinical Efficacy of Ceftriaxone in Cases of Early Forms of Syphilis
Abstract
Syphilis (lues) is a chronic infectious sexually transmitted disease, caused by a spirochete bacterium Treponema pallidum affecting all human organs. Ceftriaxone has high anti-treponemal activity and nowadays has become one of the methods of choice in treatment of syphilis.
The aim of the study was to define the efficacy of ceftriaxone in cases of primary and secondary syphilis, collecting and analysing data of Rīga 1st Hospital, Clinical Centre of Skin and Sexually transmitted Diseases, and to provide evaluation and recommendations according to clinical serological observation results of syphilis treatment by ceftriaxone.
Analysis of treatment efficacy with ceftriaxone was performed in 120 patients (62 female and 58 male, age 16–66 years), who were treated at Rīga 1st Hospital, Clinical Centre of Skin and Sexually Transmitted Diseases, in period 2008 until 2013. Nevertheless, the existing tendency of epidemiological stabilisation of morbidity, serologic resistance to specific therapy of syphilis develops often.
The therapeutic results were evaluated taking into account time of regression of clinical signs of syphilis and negativisation of serologic reactions, clinical relapses, serologic relapses and frequency of development of serologic resistance. Negativisation of serologic reactions in patients with primary syphilis was achieved in all cases in a 6-months period. In 72.3 % of luess secundaria and in 27.7 % of luess latens praecox patients stable SR negativisation was achieved in 12 months after completion of treatment course. Slowed SR negativisation was recognised in 24.4 % of luess secundaria and in 44.4 % – of luess latens praecox patients treated with ceftriaxone. The efficacy of treatment correlates with the duration of illness.
Based on the results of this project, the possibility of increasing dosage of ceftriaxone up to 1000 mg per day and extending the duration of treatment until 20 days in cases when late symptoms of syphilis appear to be considered in order to avoid the development of clinical seroresistance.
Introduction
Syphilis is a highly contagious sexually transmitted chronic infectious disease, caused by Treponema pallidum (TP). It can affect all human organs. At the onset of disease, lesions of skin and mucous membranes are present proceeding into infectious changes in lymphatic system. Degenerative alterations in visceral organs and central nervous system develop in later stages of disease. Therefore, a topical problem is improvement of specific therapy of syphilis (Starm, 2010; Psomas et al., 2012).
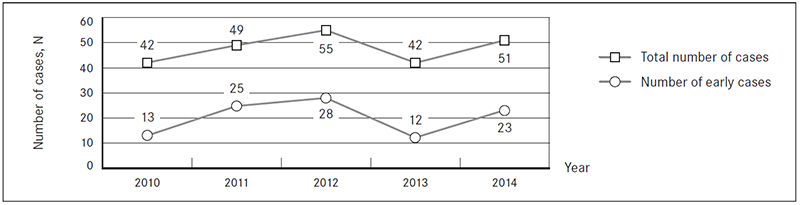
According the statistical data of Rīga 1st Hospital, Clinical Centre of Skin and Sexually Transmitted Diseases, there is a tendency of stabilisation of morbidity of syphilis per year (Table 1, Figure 1).
Table 1. Epidemiological data (for the first time registered morbidity with syphilis – number of cases per year) at Rīga 1st Hospital, Clinical Centre of Skin and Sexually Transmitted Diseases
| Year | Total number of cases, N | Number of early syphilis cases, n |
|---|---|---|
| 2010 | 42 | 13 |
| 2011 | 49 | 25 |
| 2012 | 55 | 28 |
| 2013 | 42 | 12 |
| 2014 | 51 | 23 |
Figure 1. Epidemiological data tendencies (for the first time registered morbidity with syphilis – number of cases per year) at Rīga 1st Hospital, Clinical Centre of Skin and Sexually Transmitted Diseases
Early forms of syphilis – luess primaria, luess secundaria and luess latens praecox with the duration of disease more than one year are treated ambulatory. Nevertheless, the existing tendency of epidemiological stabilisation of morbidity, serologic resistance to specific therapy of syphilis develops often. There is an obvious change in the choice of methods and tactic of treatment of syphilis during the last 5 years. In clinical praxis, there is an increase in number of anti-syphilitic drugs and tendency to decrease the duration of treatment course and the number of administering of medicines on daily bases. Moreover, in the guidelines available (Goh et al., 2001; French et al., 2009; Janier et al., 2014; Hartmane et al., 2004), there are no definite recommendations, which particular method of treatment of syphilis is to be ordinated in different new forms of syphilis, to avoid the development of clinical serological resistance. Although the tendency of last years is the use of a wider spectrum and on more frequent basis of semi-synthetic 3rd generation cephalosporin antibiotic – ceftriaxone in cases of early forms of syphilis.
Ceftriaxone has high anti-treponemal activity (www.ema.europa.eu). Its efficacy is defined by ability to suppress the synthesis of cell membrane of TP inhibiting synthesis of mucopeptides. Ceftriaxone is resistant to β-lactamases produced by TP. The main advantage of this drug to other cephalosporins of 3rd generation is its 100 % bioavailability and long period of half-life (t ½), stating the once a day regimen of administering of this drug (French et al., 2009). The treatment regimens and duration of administering of ceftriaxone differ in several available guidelines and methodological recommendations in cases of those forms of early syphilis (luess secundaria and luess latents praecox) where clinical and serological resistance develops more often (Hook et al., 2007).
Aim
The aims of this study were:
- to define the efficacy of ceftriaxone in cases of primary and secondary syphilis, collecting and analysing data of Rīga 1st Hospital, Clinical Centre of Skin and Sexually Transmitted Disease;
- to provide evaluation and recommendations regarding clinical serological observation results of syphilis treatment with ceftriaxone.
Material and Methods
Analysis of treatment efficacy with ceftriaxone was performed in 120 patients (62 female and 58 male, age 16–66 years), who were treated at Rīga 1st Hospital, Clinical Centre of Skin and Sexually Transmitted Diseases, starting from 2008 until 2013. Luess primaria was diagnosed in 7 % of patients, luess secundaria – in 78 % and luess latens praecox – in 15 % of patients, respectively. Diagnosis was based on specific clinical symptoms of syphilis and confirmed by positive serologic results (TPHA, IFA-IgG, IgM and immunoblot IgG, IgM reactions). In 9 % of secondary syphilis patients remaining clinical signs of primary syphilis period were still observed – epithelialised hard chancre and enlargement of regional lymph nodes). In case of secondary syphilis roseolas on the trunk skin were clinically observed in 28 patients (29.8 %), papules on the body surface skin – in 12 patients (12.7 %), papules on the palmar skin – in 17 patients (18 %), papules on the plantar skin – in 18 patients (19.1 %), erosive papules on the oral mucosa – in 24 patients (25.5 %), specific erythematous tonsillitis – in 8 patients (8.5 %), papules on the tongue – in 16 patients (17 %), specific laryngitis – in 5 patients (5.3 %), anogenital erosive papules – in 23 patients (24.4 %) and condylomata lata – in 14 patients (14.8 %).
In patients with condylomata lata also alopecia was recognised, which approves a belated stage of secondary syphilis. Similar to literature data, more frequent roseolas, seldom – alopecia and condylomata lata, were detected (French et al., 2009). Treatment of syphilis was administered by intramuscular injections of ceftriaxone solution 500 mg once a day for 10 days, according to the European guideline on the management of syphilis (Janier et al., 2014). Tolerability of drug was good, no allergic reactions were observed. The therapeutic results were evaluated taking into account time of regression of clinical signs of syphilis and negativisation of serologic reactions (SR), clinical relapses, serologic relapses and frequency of development of serologic resistance.
Results
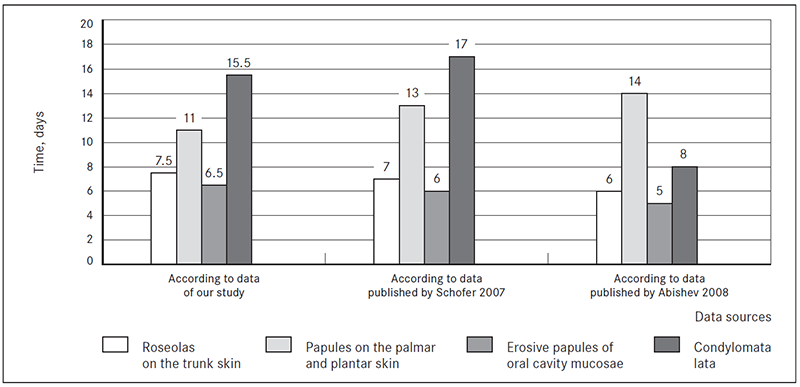
Results of treatment of syphilis were evaluated in 120 patients, presenting with early forms of syphilis, one year after treatment course with ceftriaxone. The results obtained were compared with literature data of recent years. Analysing the regression time of clinical signs of secondary syphilis, (Table 2), it was recognised that body roseolas disappeared on day 3–12, palmar and plantar papules on day 7–15, erosive papules of oral cavity mucosae on day 3–10, erosive papules of anogenital region on day 6–15, and condylomata lata on day 11–20.
The results of treatment efficacy were evaluated according to observational data of clinicalserological investigation one year and longer after completion of ceftriaxone treatment course. SR control was done according to recommendations of dynamic observation (French et al., 2009; Janier et al., 2014; Hartmane et al., 2004) once in 3 months. Data obtained are reflected in Table 3 and Figure 2.
Table 2. Regression time of clinical signs of secondary syphilis
| Clinical signs | Number of patients, n | Regression time, days (average) |
|---|---|---|
| Roseolas | 28 | 3–12 (7.5) |
| Papules on the trunk skin | 12 | 5–14 (9.5) |
| Papules on the palmar skin | 17 | 7–15 (11) |
| Papules on the plantar skin | 18 | 7–15 (11) |
| Erosive papules of oral cavity mucosae | 24 | 3–10 (6.5) |
| Specific erythematous tonsillitis | 8 | 3–10 (6.5) |
| Papules of lingual mucosae | 16 | 8–12 (10) |
| Specific laryngitis | 5 | 7–14 (10.5) |
| Erosive papules of anogenital region | 23 | 6–15 (10.5) |
| Condylomata lata | 14 | 11–20 (15.5) |
Table 3. Results of clinical-serological observation after syphilis therapy with ceftriaxone
| Results (total) (N = 120) | Luess primaria (n = 8) | Luess secundaria (n = 94) | Luess latens praecox (n = 18) |
|---|---|---|---|
| SR negativisation, n (%) | 8 (100) | 68 (72.3) | 5 (27.7) |
| Time of negativisation, months | 3–6 (average 3.6) | 3–12 (average 7.5) | 6–12 (average 9) |
| Decrease of SR positivity, n (%) | — | 23 (24.4) | 8 (44.4) |
| Clinical relapses, n | — | — | — |
| Serological relapses, n (%) | — | — | 1 (5.55) |
| Clinical relapses, n | — | — | — |
| Seroresistance, n (%) | — | 3 (3.19) | 4 (22.2) |
According to Table 3, negativisation of SR in patients with primary syphilis was achieved in all cases in a 6-month period. In 72.3 % of luess secundaria and in 27.7 % of luess latens praecox patients stable SR negativisation was achieved in 12 months after completion of treatment course. Slowed SR negativisation was recognised in 24.4 % of luess secundaria and in 44.4 % of luess latens praecox patients treated with ceftriaxone. The share of adverse results (clinical-serological relapses, seroresistance) was recognised in 3.19 % cases of luess secundaria and in 27.7 % cases of luess latens praecox (data are visualised in Figure 2). Seroresistance was confirmed in three patients with luess secundaria patients and in four of luess latens praecox patients; in one patient serological relapse developed (Table 4). In three luess secundaria patients who developed seroresistance after treatment, condylomata lata and alopecia symptoms were stated.
Figure 2. Results of clinical-serological observation after syphilis therapy with ceftriaxone
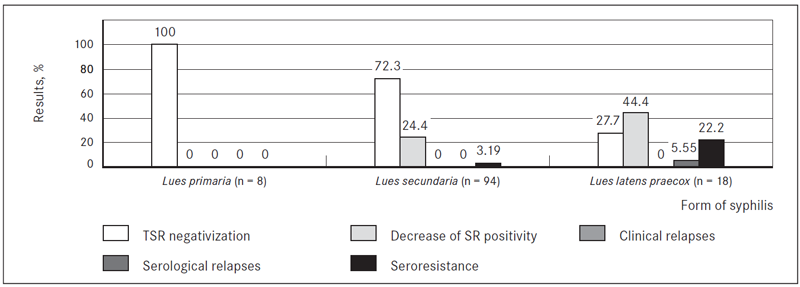
Table 4. Results of syphilis treatment with ceftriaxone
| Form of syphilis | Number of patients, n | Serological relapse, n (%) | Seroresistance, n (%) |
|---|---|---|---|
| Luess primaria | 8 | — | — |
| Luess secundaria | 94 | — | 3 |
| Luess latens praecox | 18 | 1 | 4 |
| Total | 120 | 1 (0.83) | 7 (5.8) |
Discussion
According to data published by Schofer et al. (2007), roseolas on the trunk skin regressed within 7 days from the beginning of treatment course, papules on the trunk skin within 11 days, palmar and plantar papulous lesions within 13 days, erosive papules of oral cavity and lingual mucosae within 6 days, erosive papules of anogenital region regressed within 8 days and condylomata lata persisted on average for 17 days (Figure 3).
According to data published by Abishev et al. (Абишев А. Т., 2008), the regression of syphilides occurred in the following periods: roseola – on average within 6 days, papules on the palmar and plantar skin – 13 days, erosive papules of oral cavity mucosae – 5 days and condylomata lata – 8 days (Figure 3).
The results of current study are comparable with data presented by other authors. The published data by Hook et al. (2007) and Schofer et al. (2007) report slowdown of SR negativisation for about 30 % of luess secundaria patients and in 60 % of luess latens praecox patients, as well as failures of therapy found in 3 % of patients. Psomas et al. (2012) describe total negativisation of SR in all luess secundaria patients treated with ceftriaxone in duration 5–6 months. According to their report, the regression of clinical signs of syphilis occurs more slowly, comparing with other literature data (Psomas et al., 2012; Hook et al., 2007; Schofer et al., 2007). Slower negativisation of SR was observed in one of three luess secundaria patients and in more than a half of luess latens praecox patients treated with ceftriaxone.
According to the data of our study, seroresistance was more often observed in luess secundaria and luess latens praecox cases. The data obtained are comparable with data available in literature. Taking into account that pharmacokinetic resources for treatment of syphilis, using ceftriaxone is satisfactory (French et al., 2009; Janier et al., 2014; Hartmane et al., 2004), the reasons of insufficient clinical efficacy of treatment in these cases are obviously inadequate choice of single dose and too short duration of treatment course (French et al., 2009).
Figure 3. Regression time of clinical signs of secondary syphilis
Conclusions
Conclusions were based on the data, obtained by summarising and analysing clinical information about 120 cases of early syphilis forms in patients treated with ceftriaxone, as well as performing analysis and comparison of available literature.
- Relatively faster regression of clinical symptoms and more prominent negativisation of SR were stated in patients with earlier forms of syphilis.
- Clinical-serological resistance was confirmed in 5.8 % of patients with luess secundaria and luess latens praecox.
- Serological relapse and resistance were confirmed in patients who clinically presented condylomata lata and who started to develop symptoms of alopecia.
- Based on the results of this project, the possibility to increase dosage of ceftriaxone up to 1000 mg per day and to increase the duration of treatment course until 20 days in cases when late symptoms of syphilis appear should be considered to avoid the development of clinical seroresistance.
References
- Ceftriaksons. Eiropas Zāļu aģentūra. www.ema.europa.eu
- French P., Gomberg M., Janier M., et al. IUSTI: 2008 European guidelines on the management of syphilis. Int J of STD and AIDS, 2009; 20: 300–309.
- Goh B. T., van Voorst Vader P. C. European guideline for the management of syphilis. Int J of STD and AIDS, 2001; 12, Suppl. 3: 14–26.
- Hartmane I., Mikazans I., Branta D., et al. Sifilisa ārstēšana un profilakse: metodiskie ieteikumi (eng. Treatment and Prophylaxis of Syphilis. Guidelines). Nacionālais apgāds, 2004, 5–30.
- Hook E. W., Roddy R. E., Handsfeld H. H. Ceftriaxone therapy for incubating and early syphilis. J Infect Dis, 2007; 158 (4): 881–884.
- Janier M., Hegyi V., Dupin N., et al. 2014 European guideline on the management of syphilis. EADV, 2014; 28: 1581–1593.
- Psomas K. C., Brun M., Causse A. Efficacy of ceftriaxone and doxycycline in the treatment of early syphilis. Med Mal Infect, 2012; 42 (1): 15–19.
- Starm L. V. Global challenge of antibiotic-resistant Treponema pallidum. Antimicrob Agents Chemother, 2010; 54 (2): 583–589.
- Schofer H., Vogt H. J., Milbradt R. Ceftriaxone for the treatment of primary and secondary syphilis. Chemotherapy, 2007; 35 (2): 140–145.
- Абишев А. Т. Цефтриаксон в лечении больных ранними формами сифилиса. 11 Международная конференция по первичной и вторичной профилактике инфекций, передающихся преимущественно половым путём: тезисы докладов. Бишкек, 2008, 15.



