Evaluation of Clinical Efficacy and Safety in Treatment of Patients with Moderate and Severe Forms of Psoriasis with Combined Low Dose Methotrexate and Narrow Band UVB Therapy
Abstract
Psoriasis is a chronic relapsing, genetically and immunologically associated disease. Question rises about treatment methods of psoriasis in cases when systemic therapy methods are applied, particularly, in moderate and severe cases of the disease. In routine dermatological praxis in Latvia, the novel biological medicines are not freely available for psoriasis patients; therefore, it is important to gather information and experience about such treatment methods that provide good clinical efficacy, increase safety of their administration, as, for example, application of complex methods.
The aim of the current investigation was to collect and analyse data about treatment of patients presenting with moderate and severe onset of psoriasis with a complex method, using immunosuppressing medicine methotrexate (MTX) in low doses in combination with narrow band UVB phototherapy (Nb-UVB). Retrospective analysis of patients’ medical documentation in the period between 2013 and 2016 was performed on those patients’ data, who had complete documentation on immunological investigation of blood tests at the onset and completing the therapy course. The studied patients were divided into two groups to be compared according to two main morphofunctional criteria. Patients of group 1 (n = 34) received methotrexate 10 mg s/c in regimen once a week for the period of four to six weeks and 311 nm UVB phototherapy with the initial dose 0.1–0.3 J/cm2, according the skin type and protocol of administration – three times a week; increasing the dosage in every next therapy session by 0.1–0.2 J/cm2, undergoing 10–24 procedures in the treatment course (mean 17 ± 4.2) with the total irradiation dosage 19.9 ± 3.6 J/cm2. Patients of group 2 (n = 28) were treated using methotrexate as monotherapy 2.5 mg twice a day per os for five days (total dose in the treatment course 25 mg); intervals 3–4 days; 4–6 treatment courses in total.
The obtained results show that in complex therapy in 28 (82.3 %) group 1 patients and in 12 (42.8 %) group 2 patients (MTX monotherapy) significant clinical improvement has been achieved to 80 % of the study group. In six (17.7 %) group 1 patients and nine (32.1 %) group 2 patients satisfactory improvement was achieved (PASI decrease for 79–75 %). In seven (25 %) group 2 patients a less rapid improvement was obtained (PASI 74–50 %) As the result of complex therapy, decrease of PASI at the end of the second week of the treatment in patients of group 1 was for 38 %, but in group 2 (MTX monotherapy) – for 21 %.
Complex method of moderate and severe psoriasis therapy, using MTX in low dosage and 311 nm UVB phototherapy, is clinically effective and pathogenically valid. Upon application of the complex method, rapid clinical improvement and disappearance of psoriatic lesions were detected, as well as no side effects were observed. The complex method of therapy is safe and improves the quality of patients’ lives.
Introduction
Psoriasis is a chronic relapsing, genetically and immunologically associated disease with extensive epidermal proliferation, presenting with incomplete differentiation of epidermocytes, alterations in blood vessels and infiltrates of inflammatory immunocompetent cells in epidermis and dermal papillary layer (Hartmane, 2004; Griffiths & Barker, 2007). Psoriasis has several variants of clinical expressions; it can affect joints. In case of psoriasis, differentiation of naive lymphocytes to T-helper type 1 (Th1) and T-helper type 17 (Th17) cells occur under the influence of interleukins (IL)-12 and 23, produced by activated dendritic cells. As a result, migration of Th1 and Th17 lymphocytes into skin is initiated, whereas Th1 lymphocytes induce synthesis of tumour necrosis factor – alfa (TNF-α) and gamma- interferon (γ-IFN), and Th17 lymphocytes – IL-17A–IL-17F, IL-1β, IL-6, IL-22, etc. In keratinocytes, synthesis of interleukins, haemokynes and antimicrobial peptides is activated as the result of elevated concentration of anti-inflammatory cytokines. Proliferation of keratinocytes and neoangiogenesis are accelerated, as well. Due to these processes, psoriatic skin lesions appear – papules, which are erythematous, infiltrated and presenting with desquamation and convergence, causing clinical appearance of skin lesions of different sizes, covered with silvery scales (Griffiths & Barker, 2007; European S3 guidelines, 2009; Hartmane et., 2016; Nacionālais veselības dienests, 2016).
A more pressing question arises about treatment methods of psoriasis in cases when systemic therapy methods are applied, particularly, in moderate and severe cases of the disease. In routine dermatological praxis in Latvia, the novel biological medicines are not freely available for psoriasis patients; therefore, it is important to gather information and experience about such treatment methods, which provide good clinical efficacy, increase safety of their administration, as, for example, application of complex methods (European S3 guidelines, 2009; Hartmane et al., 2016; Lebwohl et al., 2004). Nowadays, more topical is a wider administration of combined methods using systemic medications and phototherapy that simultaneously increase clinical efficacy and minimise duration period of UV irradiation in patients, decreasing risks of development of side effects (Mrowietz et al., 2014).
According to the literature data, morbidity of psoriasis in the world varies between 2 % and 4.9 % (Mrowietz et al., 2014; Hartmane et al., 2016). According to statistical data of Riga 1st hospital, in 2013 psoriasis was treated and clinically observed in 1368 patients, in 2014 – 1402 patients, in 2015 – 1497 patients and in 2016 – 1561 patients.
Aim
The aim of the current investigation was to collect and analyse data about treatment of patients presenting with moderate and severe onset of psoriasis with combined method, using immunosuppressing medicine methotrexate (MTX) in low doses in combination with narrow band UVB phototherapy (Nb-UVB), as well as provide recommendations according to the obtained results about practical application of this method in dermatological praxis.
Material and Methods
Retrospective analysis of patients’ medical documentation in the period between 2013 and 2016 was performed on those patients’ data who had complete documentation on immunological investigation of blood tests at the onset and completing the therapy course. Thereby, data on 62 patients with moderate form of psoriasis were gathered. There were 32 female and 30 male patients aged 22–64, whose duration of the disease varied between 8 and 23 years. Psoriasis area and severity index (PASI) varied from 30.2 ± 7.3.
Severity of the disease, according to PASI, was determined as follows:
- mild to moderate form – area of psoriatic lesions < 10 % or PASI < 10 %;
- moderate to severe form – area of psoriatic lesions > 10 % or PASI > 10 %;
- moderately severe to severe form – area of psoriatic lesions > 10 % or PASI 10–20 %;
- severe form – area of psoriatic lesions > 20 % or PASI > 20 % (Nacionālais veselības dienests, 2016).
Psoriatic patients included in the analysis were treated with combined method, applying narrow band UVB 311 nm phototherapy and methotrexate. In psoriasis, phototherapy has immunosuppressive influence on functions of antigen-presenting cells and production of cytokines. It induces apoptosis also in pathogenically significant cells. In phototherapy, the dosage is determined according to the phototype of patient’s skin. Inception dosage is 0.1–0.3 J/cm2 2–5 times per week, in treatment course of 25 procedures (Goktas et al., 2006; Menter et al., 2010). According to the literature data, methotrexate is one of the most effective medicines in cases of vastly spread skin and joint forms of psoriasis (European S3 guidelines, 2009; Mrowietz et al., 2014). In psoriasis, low dosages methotrexate is used as anti-inflammatory and immunomodulatory treatment. It stimulates release of adenosine in psoriatic lesion, decreases release of leukotrienes, tumour necrotic factor α (TNF- α) and other cytokines, as well as provide the switching of synthesis of cytokines from Th1 (IL-2, γ-interferons) to Th2 (IL-10). Advantage of the use of methotrexate is determined by different options of its administration: per os, intramuscular and subcutaneously. In case of psoriasis, this medication is used in mean dosage 15 mg per week (Asawanonda & Nateetongrungsak, 2006; Mrowietz et al., 2014). Among systemic drugs used in psoriasis therapy, by means of efficacy, only biological preparations are more effective than methotrexate. Although, there are cases when methotrexate is used both as start-up therapy before the biological medicaments, and in combination with them (Schmitt et al., 2008).
Analysed patients were divided in two groups to be compared according to two main morphofunctional criteria. Patients of group 1 (n = 34) received methotrexate 10 mg s/c in regimen once a week for 4 to 6 weeks and 311 nm UVB phototherapy with the initial dose 0.1–0.3 J/cm2, according to skin type and protocol of administration – three times a week; increasing the dosage in every next therapy session by 0.1–0.2 J/cm2, undergoing 10–24 procedures in the treatment course (mean 17 ± 4.2) with the total irradiation dosage 19.9 ± 3.6 J/cm2. Patients of group 2 (n = 28) were treated, using methotrexate as monotherapy 2.5 mg two times a day per os for the period of five days (total dose in the treatment course 25 mg); intervals 3–4 days, 4–6 treatment courses in total. Morphologic and functional criteria, according to which the selection of psoriasis patients was performed included PASI and in laboratory tests approved alterations of complimentary to psoriasis immunologic parameters – lymphocytes CD3+, CD4+, CD8+, CD3 HLA-DR. PASI was applied to evaluate the objective clinical improvement during therapy. Immunological parameters, in turn, allow analysing the efficacy of the administered methods of treatment on the pathogenetical events in psoriasis disease.
Due to the data being analysed retrospectively, patients were divided into groups according to the randomness principle. In both groups, the number of patients was equal according to age and gender. The relevance of normal distribution of both groups of selected patients was confirmed by non-parametrical test of Kolmogorov-Smirnov for analysis of one selection, as well as by graphical curves P-P and Q-Q of percentiles and quartiles. For the comparison of data the T test for confrontation of two independent selections was applied.
According to medical documentation, all patients had to undergo digital dermatoscopy investigation, to exclude possibility of malignant skin lesions, as well as blood tests and biochemical investigation of blood to evaluate the functions of liver and kidneys.
Results and Discussion
The efficacy of the complex therapy with MTX and 311 nm UVB phototherapy was evaluated as follows:
- obvious improvement – PASI decrease by 80 %;
- moderate improvement – PASI decrease by 79–75 %;
- improvement – PASI decrease by 74–50 %;
- no effect – PASI decrease less than 50 %;
- worsening – remaining of negative dynamics or regression of the pathological process.
As the result of complex therapy, decrease of PASI at the end of the 2nd week of treatment in patients of group 1 was by 38 %, but in group 2 (MTX monotherapy) – by 21 %. Hereafter, less but more stable decrease of PASI was detected (see Figure 1). At the end of the therapeutic course (4–6 weeks) PASI in group 1 reached 5.3 ± 0.2 (p < 0.01) and in group 2 – 8.4 ± 0.7. Decrease of PASI in group 1 was determined on average by 80 %, but in group 2 – by 68 %.
The obtained results show that in complex therapy in 28 (82.3 %) group 1 patients and in 12 (42.8 %) group 2 patients (MTX monotherapy), a significant clinical improvement has been achieved by 80 %. In 6 (17.7 %) group 1 patients and 9 (32.1 %) group 2 patients, a satisfactory improvement was achieved (PASI decrease by 79–75 %). In 7 (25 %) group 2 patients, a less rapid improvement was obtained (PASI 74–50 %) (see Figure 2).
It must be admitted that in those patients who were treated with MTX, the therapeutic efficacy was lower than in those patients who received the complex therapy. In group 1 patients treated with the complex method, side effects or complications were not observed, approving the high safety of the method. In group 2, temporary side effects such as nausea, headache, elevated ALAT in plasma and moderate thrombocytopenia were documented in six patients.
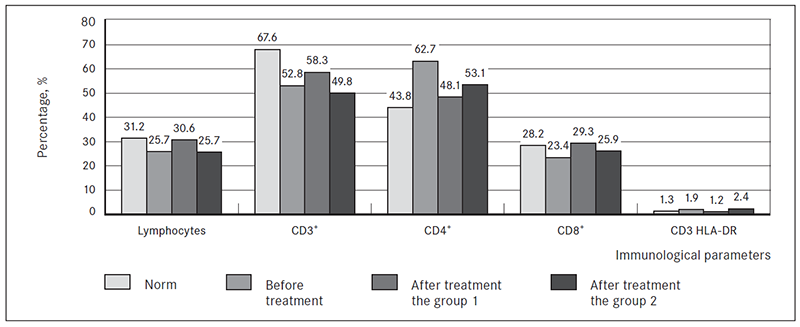
Analysis of this investigation demonstrates that before the start of therapy, the immunoregulatory alterations in psoriasis patients are characterised with elevated concentration of T-helper (Th) lymphocytes in blood serum, which determine the inflammatory reaction and the decreased level of cytotoxic T lymphocytes (CD3+) in the background of the decreased total number of T lymphocytes. In patients who received the complex therapy, normalisation of the immunoregulatory parameters of cell immunity were defined after the treatment course, such as lowering of the Th level and increasing of concentration of cytotoxic T lymphocytes in blood. Content of the activated CD3/HLA-DR cells after therapy showed no significant alterations and remained within the normal range (see Figure 3).
Figure 1. Data of therapeutic efficacy of complex treatment method in comparison with 311 nm UVB and MTX monotherapy
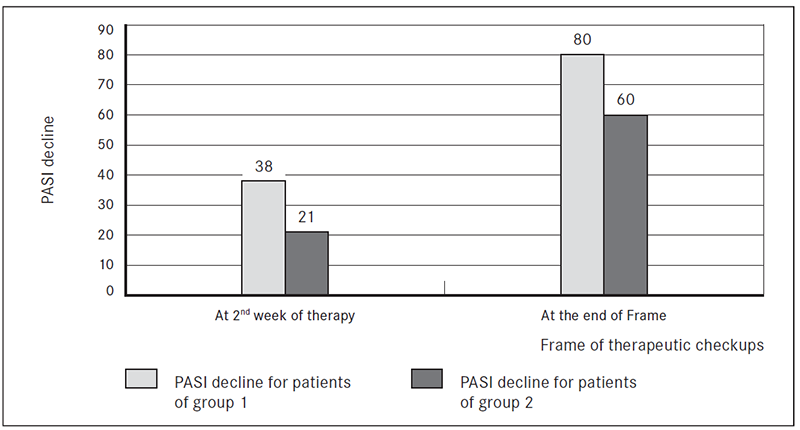
Figure 2. Changes of PASI in psoriasis patients after complex therapy (group 1) and MTX monotherapy (group 2) course
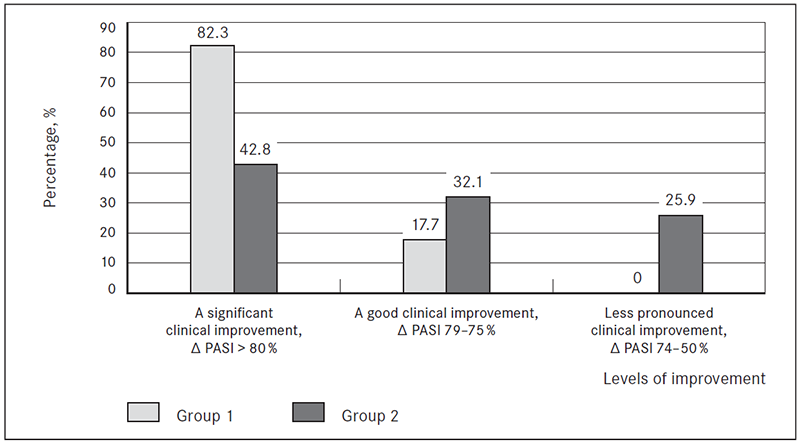
Figure 3. Immunological parameters in psoriasis patients before and after therapy
Conclusions
- Complex method of moderate and severe psoriasis therapy, using MTX in low dosage and 311 nm UVB phototherapy, is clinically effective and pathogenically valid.
- Applying the complex method, rapid clinical improvement and disappearance of psoriatic lesions were detected, as well as no side effects were observed.
- Complex method of therapy is safe and improves the quality of patients’ lives.
References
- Asawanonda, P., Nateetongrungsak, Y. 2006. Methotrexate plus narrowband UVB phototherapy vs. narrowband UVB phototherapy alone in the treatment of plaque-type psoriasis: a randomised, placebo-controlled study. J Am Acad Dermatol. 54, 1013–1018.
- European S3 guidelines in the systemic treatment of psoriasis vulgaris. 2009. JEADV. 30 (2), 5–70.
- Goktas, E., Aydin, F., Senturk, N. et al. 2006. Mechanism of ultraviolet (UV) B and UVA phototherapy. JEADV. 20, 553–557.
- Griffiths, C. E., Barker, J. N. 2007. Pathogenesis and clinical features of psoriasis. Lancet. 370, 263–271.
- Hartmane, I. 2004. Psoriāze (Eng. Psoriasis). Rīga, 2004.
- Hartmane, I., Mikazans, I., Ivdra, I., Derveniece, A. et al. 2016. Experience of phototherapy in dermatological praxis in complex therapy of psoriasis patients. Proc Latv Acad Sci. 70, 7–12.
- Lebwohl, M., Menter, A., Koo, J., Feldman, S. R. 2004. Combination therapy to treat moderate to severe psoriasis. J Am Acad Dermatol. 50, 416–430.
- Menter, A., Korman, N. J., Elmets, C. A., Feldman, S. R. et al. 2010. Guidelines of care for the treatment of psoriasis with phototherapy and photochemotherapy. J Am Acad Dermatol. 62, 114–135.
- Mrowietz, U., de Jong, E. M. G. J., Kragballe, K. et al. 2014. A consensus report on appropriate treatment optimization and transitioning in the management of moderate-to severe plaque psoriasis. JEADV. 28, 438–453.
- Nacionālais veselības dienests. 2016. Vidēji smagas un smagas gaitas psoriāzes klīniskās vadlīnijas. Klīniskās vadlīnijas. Klīnisko vadlīniju datu bāze; reģistrētas 2016. gadā (Eng. Clinical guidelines for moderate to severe psoriasis. Clinical guidance database; registered in 2016). Available from: www.vmnvd.gov.lv [viewed 30.09.2017].
- Schmitt, J., Zhang, Z., Wozel, G. et al. 2008. Efficacy and tolerability of biologic and non-biologic systemic treatments for moderate to severe psoriasis: meta-analysis of randomised controlled trials. Br J Dermatol. 159, 513–526.



