EEG Controlled Sedation in Patients Undergoing Hand Surgery under Regional Anaesthesia: Dexmedetomidine vs. Propofol Target Controlled Infusion
Abstract
The aim of the study is to compare sedations with dexmedetomidine vs. propofol controlled by Narcotrend electroencephalogram (EEG) in patients undergoing hand surgery under regional anaesthesia.
50 patients ASA I–II undergoing hand surgery under brachial plexus block, included in a prospective study, were randomised into 2 groups of 25.
Sedation with dexmedetomidine: a loading dose 1 μg/kg over 10 min, followed by infusion 0.1–0.6 μg/kg/h.
Sedation with propofol: Target Controlled Infusion (TCI), using Schnider Effect Site pharmacokinetic model, initial dose: 2.5 μg/ml.
Sedation depth was controlled with EEG index by Narcotrend.
After 10 minutes of sedation with dexmedetomidine patients’ heart rate (HR) decreased from 74.9 ± 10.0 to 62.8 ± 7.9 ×/min (p < 0.01), systolic blood pressure (SBP) decreased from 136.7 ± 22.2 to 122.5 ± 17.7 mmHg (p < 0.01), diastolic blood pressure (DBP) decreased from 82.7 ± 14.3 to 72.5 ± 11.1 mmHg (p < 0.01).
After 10 minutes of sedation with propofol patients’ HR decreased from 74.1 ± 13.1 to 71.2 ± 10.6 ×/min (p = 0.15), SBP decreased from 139.2 ± 19.4 to 128.6 ± 19.5 mmHg (p < 0.01), DBP decreased from 84.1 ± 14.6 to 76.0 ± 14.5 mmHg (p < 0.01).
Mean haemodynamic values during surgery in dexmedetomidine group: HR 61.7 ± 7.5, SBP 120.7 ± 38.3, DBP 70.3 ± 10.4 and in propofol group: HR 69.4 ± 11.5, SBP 121.6 ± 19.6, DBP 71.8 ± 14.7.
All patients in both groups maintained spontaneous breathing, no patient required bag-mask ventilation. To maintain SpO2 > 95 % in dexmedetomidine group 48 % patients required O2, no patient required oral airway insertion or jaw thrust; in propofol group 56 % required O2, no patient required oral airway insertion but 20 % required jaw thrust.
Sedation with dexmedetomidine decreased patients’ heart rate more than sedation with propofol (p < 0.01) but did not require treatment. There was no difference in blood pressure values between both groups.
Patients sedated with dexmedetomidine required achievement of correct airway less frequently than patients sedated with propofol (p = 0.02).
Introduction
Sedation is widely used during regional anaesthesia in order to reduce patients’ stress and discomfort from being awake while lying on the operating table [17]. During sedation in patients undergoing regional anaesthesia, it is important to keep a patient drowsy, light or moderate sedated to maintain spontaneous breathing, which is a hard task.
The latest sedative in clinical practice is dexmedetomidine [12, 19, 23, 33] it is highly selective α2 receptor agonist with sedative, anxiolytic and analgesic effect. Dose dependent bradycardia and hypotension are the most frequently reported adverse effects of dexmedetomidine sedation [10, 11, 20, 22, 24, 27] but without respiratory depression [2, 15, 19, 24, 25, 28].
Aim
The aim of this study was to compare sedation with dexmedetomidine vs. sedation with propofol in patients undergoing hand surgery under regional anaesthesia. We evaluated influence of two different methods of sedation on respiratory function, haemodynamics and registered side effects.
Material and Methods
In a prospective cohort study 50 patients ASA I–II over the age of 18 undergoing brachial plexus block for hand surgery were randomly allocated in 2 groups of 25 patients to receive sedation with dexmedetomidine or propofol. The study was approved by Rīga Stradiņš University ethical committee on 26.02.2015 and Riga Eastern Clinical University Hospital ethical committee on 02.02.2015. All patients provided a written consent to participate.
The exclusion criteria we used were patients with cardiovascular diseases, liver failure, pregnancy, sleep or mental disorders.
Anaesthesia methods. All patients in both groups received premedication with midazolam 7.5 mg before surgery. For brachial plexus blockade 20 ml 0.5 % bupivacaine and 20 ml 1 % lidocaine were used for hand reconstructive surgeries without exceeding the maximum recommended doses of local anaesthetics.
Sedation method with dexmedetomidine. A loading dose of 1μg/kg over 10 min, followed by infusion of 0.1–0.6 μg/kg/h, controlled by Narcotrend electroencephalogram (EEG) index of 50–70.
Sedation method with propofol. Target Controlled Infusion (TCI), using Schnider Effect Site pharmacokinetic model with initially set dose of 2.5 μg/ml adjusted during surgery (1–4 μg/ml) controlled by Narcotrend EEG index of 50–70. TCI is a computer-driven system that manages infusion according to on-previous studies based pharmacokinetic model [4, 6].
Monitoring. Standard monitoring was used during sedation: heart rate (HR), non-invasive systolic (SBP) and diastolic (DBP) blood pressure, respiratory rate (RR), peripheral oxygen saturation (SpO2). Bradycardia was defined as HR < 50 beats per minute for more than 5 minutes. Respiratory depression was defined as RR < 12 breaths per minute or SpO2 < 90 %. For patients with decreased SpO2 we used airway obstruction management algorithm (Figure 1) [8].
Electroencephalogram monitoring using Narcotrend EEG monitor was performed for all patients in both groups during sedation. The monitor recorded patients’ hypnotic status and the depth of sedation, and classified EEG stages on a scale from A to F (Table 1), referring to a range of EEG indexes [5, 18].
Level of sedation was measured by Richmond Agitation Sedation Scale (RASS) (Table 2) [26] before sedation, after first 10 minutes of sedation and every 10 minutes until the end of surgery. The optimal sedation level was considered RASS −2 or −3 [26, 29].
Patients’ satisfaction with the received sedation and recovery was evaluated from handed out questionnaires an hour after the end of surgery.
Data statistical analysis was performed using IBM SPSS Statistics and Microsoft Excel. Kolmogorov–Smirnov and Shapiro–Wilk tests were used to determine normality of distribution. To evaluate data Student’s T test, Chi-Square test and Mann–Whitney test were used.
Figure 1. Management of airway obstruction for sedation
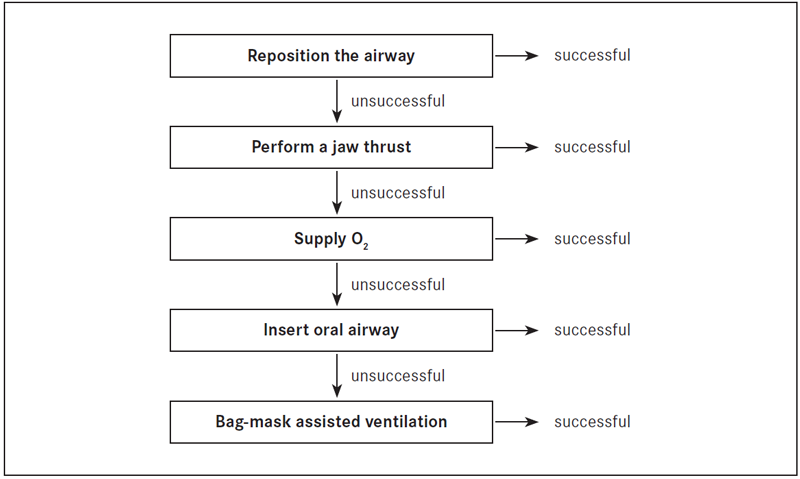
Table 1. Narcotrend EEG index and stages
| EEG index | EEG stage | Clinical condition |
|---|---|---|
| 95–100 | A | Awake |
| 80–94 | B | Sedated |
| 65–79 | C | Light anaesthesia |
| 37–64 | D | General anaesthesia |
| 13–36 | E | General anaesthesia with deep hypnosis |
| 0–12 | F | General anaesthesia with increasing burst suppression |
Table 2. Richmond Agitation Sedation Scale
| +4 | Combative | Overtly combative or violent, immediate danger to staff |
|---|---|---|
| +3 | Very agitated | Pulls on or removes tubes or catheters or has aggressive behaviour towards staff |
| +2 | Agitated | Frequent no purposeful movements |
| +1 | Restless | Anxious or apprehensive but movements not aggressive or vigorous |
| 0 | Alert and calm | — |
| -1 | Drowsy | Not fully alert, but has sustained (more than 10 seconds) awakening, with eye contact/eye opening to voice |
| -2 | Light sedation | Briefly (less than 10 seconds) awakens with eye contact to voice |
| -3 | Moderate sedation | Any movement (but no eye contact) to voice |
| -4 | Deep sedation | No response to voice, but any movement to physical stimulation |
| -5 | Unarousable | No response to voice or physical stimulation |
Results
There was no significant difference in demographic and surgical characteristics between patients in both groups (Table 3).
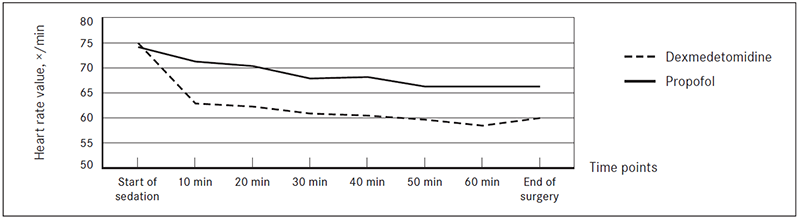
After 10 min of sedation with dexmedetomidine patients’ mean HR decreased from 74.9 ± 10.0 to 62.8 ± 7.9 ×/min (−16.2 %, p < 0.01), during surgery in patients sedated with dexmedetomidine mean HR value was 61.7 ± 7.5 ×/min (Table 4).
After 10 min of sedation with propofol patients’ HR decreased from 74.1 ± 13.1 to 71.2 ± 10.6 ×/min (−3.9 %, p = 0.15), during surgery in patients sedated with propofol mean HR value was 69.4 ± 11.5 ×/min (Table 4).
No patient sedated with either dexmedetomidine or propofol had HR below 50 ×/min (Figure 2).
Table 3. Demographic data and surgical characteristics
| Valuable | Dexmedetomidine group | Propofol group | p value * |
|---|---|---|---|
| Gender – Female : male, n (%) | 9 (36 %) : 16 (64 %) | 10 (40 %) : 15 (60 %) | 0.77 |
| Mean age, years | 46.6 ± 15 | 52 ± 15 | 0.59 |
| Mean body mass, kg | 76.0 ± 15.4 | 74.5 ± 12.8 | 0.71 |
| Body mass index, kg/m2 | 25 ± 4.3 | 25.1 ± 4.6 | 0.94 |
| Type of surgery – elective : acute | 22 (88 %) : 3 (12 %) | 19 (76 %) : 6 (24 %) | 0.27 |
| Mean duration of surgery, min | 81 ± 57.8 | 64 ± 33.4 | 0.21 |
* p – significance of difference between both groups.
Table 4. Changes in HR during sedation
| Dexmedetomidine | n | SM | SD | Propofol | n | SM | SD | SM difference | p value |
|---|---|---|---|---|---|---|---|---|---|
| Start of sedation | 25 | 74.9 | 10.0 | Start of sedation | 25 | 74.1 | 13.1 | 0.8 | 0.81 |
| 10 min | 25 | 62.8 | 7.9 | 10 min | 25 | 71.2 | 10.6 | -8.4 | 0.00 |
| 20 min | 25 | 62.2 | 7.7 | 20 min | 25 | 70.3 | 13.0 | -8.1 | 0.01 |
| 30 min | 25 | 60.8 | 6.8 | 30 min | 23 | 67.8 | 12.0 | -6.9 | 0.02 |
| 40 min | 23 | 60.4 | 7.2 | 40 min | 22 | 68.1 | 10.6 | -7.7 | 0.01 |
| 50 min | 19 | 59.6 | 6.0 | 50 min | 17 | 66.2 | 11.8 | -6.7 | 0.04 |
| 60 min | 15 | 58.4 | 5.9 | 60 min | 12 | 66.2 | 11.1 | -7.8 | 0.04 |
| End of surgery | 25 | 59.9 | 6.7 | End of surgery | 25 | 66.2 | 10.2 | 6.2 | 0.04 |
| Mean value | 25 | 61.7 | 7.5 | Mean value | 25 | 69.4 | 11.5 | -7.5 | 0.01 |
n – number of patients; SM – statistic mean; SD – standard deviation.
Figure 2. Heart rate values
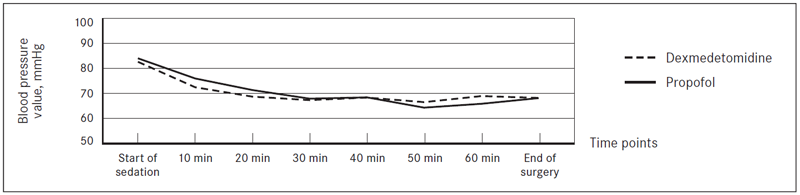
After 10 min of sedation with dexmedetomidine patients’ mean SBP decreased from 136.7 ± 22.2 to 122.5 ± 17.7 mmHg (−10.4 %, p < 0.01), mean DBP decreased from 82.7 ± 14.3 to 72.5 ± 11.1 mmHg (−12.3 %, p < 0.01). During surgery in patients sedated with dexmedetomidine mean SBP value was 120.6 ± 38.3 mmHg (Table 5), and mean DBP value was 70.3 ± 10.4 (Table 6).
After 10 min of sedation with propofol patients’ mean SBP decreased from 139.2 ± 19.4 to 128.6 ± 19.5 mmHg (−8.6 %, p < 0.01), mean DBP decreased from 84.1 ± 14.6 to 76.0 ± 14.5 mmHg (−9.6 %, p < 0.01). During surgery in patients sedated with propofol mean SBP value was 121.6 ± 19.6 mmHg (Table 5), and mean DBP value was 71.8 ± 14.7 (Table 6).
There was no significant difference between SBP (Table 5, Figure 3) and DBP (Table 6, Figure 4) values in patients sedated with dexmedetomidine and patients sedated with propofol.
Table 5. Changes in SBP during sedation
| Dexmedetomidine | n | SM | SD | Propofol | n | SM | SD | SM difference | p value |
|---|---|---|---|---|---|---|---|---|---|
| Start of sedation | 25 | 136.7 | 22.2 | Start of sedation | 25 | 139.2 | 19.4 | -2.5 | 0.67 |
| 10 min | 25 | 122.5 | 17.7 | 10 min | 25 | 128.6 | 19.5 | -6.2 | 0.25 |
| 20 min | 25 | 114.4 | 14.3 | 20 min | 25 | 121.4 | 18.5 | -7.0 | 0.14 |
| 30 min | 25 | 112.9 | 13.1 | 30 min | 23 | 116.0 | 16.3 | -3.0 | 0.48 |
| 40 min | 23 | 111.0 | 11.0 | 40 min | 22 | 113.7 | 15.1 | -2.7 | 0.49 |
| 50 min | 19 | 109.4 | 10.5 | 50 min | 17 | 113.4 | 14.8 | 4.0 | 0.28 |
| 60 min | 15 | 115.7 | 12.8 | 60 min | 12 | 112.5 | 9.1 | -3.2 | 0.58 |
| End of surgery | 25 | 122.5 | 17.7 | End of surgery | 25 | 118.2 | 16.6 | 3.8 | 0.34 |
| Mean value | 25 | 120.6 | 38.3 | Mean value | 25 | 121.6 | 19.6 | -1.0 | 0.79 |
n – number of patients; SM – statistic mean; SD – standard deviation.
Figure 3. Systolic blood pressure values
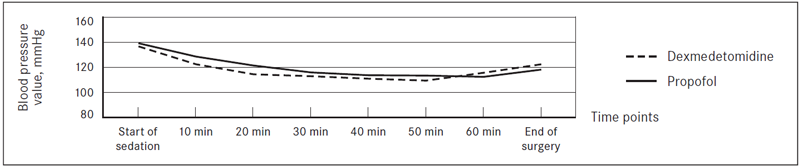
Table 6. Changes in DBP during sedation
| Dexmedetomidine | n | SM | SD | Propofol | n | SM | SD | SM difference | p value |
|---|---|---|---|---|---|---|---|---|---|
| Start of sedation | 25 | 82.7 | 14.3 | Start of sedation | 25 | 84.1 | 14.6 | -1.4 | 0.73 |
| 10 min | 25 | 72.5 | 11.1 | 10 min | 25 | 76.0 | 14.5 | -3.5 | 0.34 |
| 20 min | 25 | 68.8 | 10.5 | 20 min | 25 | 71.4 | 14.0 | -2.7 | 0.45 |
| 30 min | 25 | 67.4 | 9.0 | 30 min | 23 | 68.0 | 13.6 | -0.7 | 0.84 |
| 40 min | 23 | 68.4 | 8.7 | 40 min | 22 | 68.5 | 12.2 | -0.1 | 0.97 |
| 50 min | 19 | 66.6 | 7.4 | 50 min | 17 | 64.4 | 10.2 | 2.2 | 0.46 |
| 60 min | 15 | 69.0 | 7.6 | 60 min | 12 | 65.9 | 9.4 | 3.1 | 0.35 |
| End of surgery | 25 | 68.3 | 7.8 | End of surgery | 25 | 68.2 | 13.5 | 0.1 | 0.97 |
| Mean value | 25 | 70.3 | 10.4 | Mean value | 25 | 71.8 | 14.7 | -1.5 | 0.35 |
n – number of patients; SM – statistic mean; SD – standard deviation.
Figure 4. Diastolic blood pressure values
In patients sedated with dexmedetomidine mean RR values were similar at the start of sedation (14.8 ± 1.2 ×/min) and after 10 minutes of sedation (14.6 ± 1.4 ×/min) (Table 7).
After 10 minutes of sedation with propofol, patients’ RR decreased from 16.0 ± 2.2 to 14.5 ± 1.7 ×/min (−9.4 %, p < 0.01), during surgery in patients sedated with propofol mean RR value was 14.6 ± 1.8 ×/min (Table 7).
There was no significant difference between RR values in patients sedated with dexmedetomidine and patients sedated with propofol (Table 7, Figure 5).
All patients in both groups maintained spontaneous breathing; no patient required bag-mask ventilation.
To maintain SpO2 > 95 % in dexmedetomidine group, 48 % patients required O2 supply; no patient required oral airway insertion or jaw thrust; in propofol group 56 % required O2 supply; no patient required oral airway insertion, but 20 % required jaw thrust (Figure 6).
Table 7. Changes in RR during sedation
| Dexmedetomidine | n | SM | SD | Propofol | n | SM | SD | SM difference | p value |
|---|---|---|---|---|---|---|---|---|---|
| Start of sedation | 25 | 14.8 | 1.2 | Start of sedation | 25 | 16.0 | 2.2 | -1.20 | 0.02 |
| 10 min | 25 | 14.6 | 1.4 | 10 min | 25 | 14.5 | 1.7 | 0.12 | 0.79 |
| 20 min | 25 | 14.0 | 1.3 | 20 min | 25 | 14.5 | 1.7 | -0.48 | 0.25 |
| 30 min | 25 | 14.0 | 1.4 | 30 min | 23 | 14.6 | 1.8 | -0.56 | 0.21 |
| 40 min | 23 | 14.2 | 1.3 | 40 min | 22 | 14.7 | 1.8 | -0.41 | 0.36 |
| 50 min | 19 | 14.1 | 1.1 | 50 min | 17 | 14.3 | 1.5 | -0.14 | 0.58 |
| 60 min | 15 | 14.0 | 1.6 | 60 min | 12 | 15.0 | 2.1 | -1.00 | 0.22 |
| End of surgery | 25 | 14.1 | 1.4 | End of surgery | 25 | 14.8 | 2.7 | -0.62 | 0.86 |
| Mean value | 25 | 14.2 | 1.3 | Mean value | 25 | 14.6 | 1.8 | -0.40 | 0.40 |
n – number of patients; SM – statistic mean; SD – standard deviation.
Figure 5. Respiratory rate during sedation
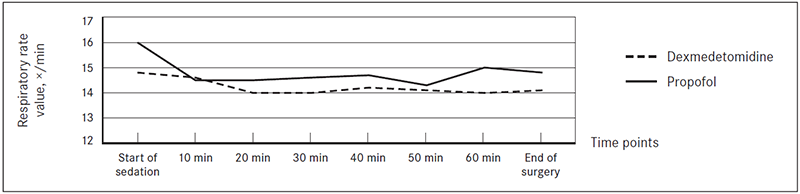
Figure 6. Actions required to maintain SpO2 > 95 %
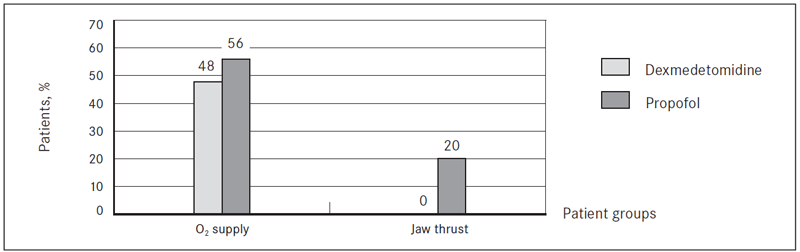
Patients sedated with dexmedetomidine required achievement of correct airway less frequently than patients sedated with propofol, (0 % vs. 20 %, p = 0.02).
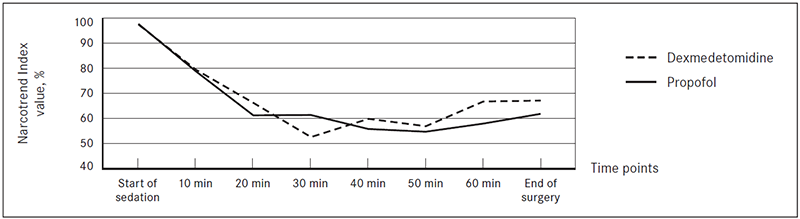
After 10 minutes of sedation with dexmedetomidine patients’ mean Narcotrend EEG Index (NI) decreased to 79.3 ± 22.4 (−20.7 %, p < 0.01), during surgery in patients sedated with dexmedetomidine mean NI value was 63.8 ± 26.3 (Table 8).
After 10 minutes of sedation with propofol patients’ mean NI decreased to 78.5 ± 1.7 (−21.5 %, p < 0.01), during surgery in patients sedated with propofol mean NI value was 61.8 ± 20.2 (Table 8).
Target depth of sedation of 50–70 NI was achieved within 10 minutes and maintained in both groups (Table 8, Figure 7). There was no significant difference between NI values in patients sedated with dexmedetomidine and patients sedated with propofol within first 50 minutes of sedation.
Table 8. NI values during sedation
| Dexmedetomidine | n | SM | SD | Propofol | n | SM | SD | SM difference | p value |
|---|---|---|---|---|---|---|---|---|---|
| Start of sedation | 25 | 97.2 | 2.0 | Start of sedation | 25 | 97.5 | 3.6 | 0.30 | 0.98 |
| 10 min | 25 | 79.3 | 22.4 | 10 min | 25 | 78.7 | 18.8 | -0.60 | 0.56 |
| 20 min | 25 | 66.1 | 25.8 | 20 min | 25 | 61.2 | 19.5 | -4.80 | 0.46 |
| 30 min | 25 | 52.6 | 24.8 | 30 min | 23 | 58.4 | 18.7 | 5.80 | 0.32 |
| 40 min | 23 | 59.8 | 26.4 | 40 min | 22 | 61.4 | 19.4 | 1.60 | 0.80 |
| 50 min | 19 | 56.9 | 26.6 | 50 min | 17 | 55.8 | 18.8 | -1.10 | 0.86 |
| 60 min | 15 | 66.7 | 27.8 | 60 min | 12 | 54.7 | 18.3 | -12.0 | 0.01 |
| End of surgery | 25 | 67.1 | 22.8 | End of surgery | 25 | 57.9 | 18.9 | -9.20 | 0.01 |
| Mean value | 25 | 63.8 | 26.3 | Mean value | 25 | 61.8 | 20.2 | 2.0 | 0.49 |
n – number of patients; SM – statistic mean; SD – standard deviation.
Figure 7. Narcotrend Index during sedation
Patients sedated with Dexmedetomidine were arousable by moderate noises in operating room during surgery, they were briefly awakening and falling back asleep without necessity to increase dexmedetomidine dose; but to patients sedated with propofol, Narcotrend Index values were resistant to similar noises during surgery.
According to answers from their questionnaires, all patients in both groups were satisfied with the received sedation.
Discussion
Different sedatives: midazolam, diazepam, propofol and barbiturates are used for sedation during regional anaesthesia in order to reduce patients’ stress and discomfort from being awake while lying on the operating table [17]. During sedation, it is important keep patient sleeping and maintain spontaneous breathing, which is a difficult task. The latest sedative in clinical practice is dexmedetomidine [2, 19, 23, 28]; there are only few reports about dexmedetomidine use during regional anaesthesia.
Literature describes that dexmedetomidine is not associated with significant respiratory depression [3, 14, 31, 32], this is why it has been hypothesised for propofol sedation to be a good alternative to be widely used in clinical practice.
Dose dependent bradycardia and hypotension are the most frequently reported adverse effects of dexmedetomidine [10, 11, 20, 22, 27]. Bradycardia is mainly associated with rapid bolus dose infusion that exceeds 1 μg/kg/h over 10 minutes [22]. Dexmedetomidine causes biphasic blood pressure reaction: short hypertension phase caused by α2B adrenal receptor activation followed by hypotension phase caused by α2A adrenal receptor activation [19, 32].
There are different methods described of dexmedetomidine administration for sedation. All of these methods start with bolus dose over 10 minutes, to avoid bradycardia that is associated with rapid infusion of dexmedetomidine.
Arain S. R. and Ebert T. J. described dexmedetomidine bolus dose of 1 μg/kg over 10 minutes followed by infusion of 0.4–0.7 μg/kg/h, as safe and sufficient for sedation [2]. Kilic N. et al. used dexmedetomidine bolus dose of 1 μg/kg over 10 minutes followed by infusion of 0.5–0.7 μg/kg/h providing adequate sedation and suggested dexmedetomidine as a better alternative to midazolam. [21]. In the current, study sedation with either dexmedetomidine or propofol did not cause treatment requiring bradycardia. There were two patients that had a brief heart rate decrease below 50 beats per minute (not < 45 ×/min). Those were young patients without existing cardiac co morbidities. Heart rate decreases were self-limited – did not exceed 5 minutes and did not require treatment with atropine.
Some authors describe dexmedetomidine as a useful sedative because of its minimal respiratory depression [7, 9]. Belleville J. P. et al. reported a study of respiratory effects of four different doses over twominute infusion; results showed that exceeding the maximum dose of 2.0 μg/kg irregular breathing with periods of apnoea were noticed but there was no significant arterial oxygen desaturation below 90 % [30].
In our study, the depth of sedation was controlled by Narcotrend EEG monitor, maintaining target level of Narcotrend index of 50–70 and Richmond agitation sedation scale level of −2 to −3. Although interpretation of assessment scales are subjective, and cannot be used in real time, authors describe them as an effective addition to neuromonitoring [24]. Narcotrend EEG monitoring was described effective to provide more accurate sedative dose adjustment [18].
Propofol sedation method was a target controlled infusion, which is described as superior to intermittent bolus dose infusion [16] and manual infusion [1, 16] because of its precision and safety. The most commonly used pharmacokinetic models at the moment are Marsch’s and Schnider’s effect site. Marsch’s model infuses significantly bigger bolus dose to achieve required target concentration, which makes Schnider’s effect site model to be safer especially in old patient population and for patients with impaired respiratory functions with increased risks of hypoxemia [4, 13]. We used Schnider’s effect site pharmacokinetic model because it is newer, uses more patient related variables, e.g. age, allometric body mass, lean body mass and height, and provides smoother bolus dose infusion.
Patients sedated with dexmedetomidine were arousable by moderate noises in operating room during surgery, they were briefly awakening and falling back asleep without nesissity to increase dexmedetomidine dose; but to patients sedated with propofol, Narcotrend Index values were resistant to similar noises during surgery. It is described that patients sedated with dexmedetomidine are easily arousable without suppression in cognitive or motor functions [21], and results of our study confirmed this effect.
Conclusions
- Sedation with dexmedetomidine in patients undergoing hand surgery under regional anaesthesia decreased patients’ heart rate significantly more than sedation with propofol (p < 0.01); however, there was no observed incidence of bradycardia or hypotension that required treatment.
- Patients sedated with dexmedetomidine required achievement of correct airway less frequently than patients sedated with propofol (p = 0.02).
- Sedation with dexmedetomidine using a loading dose 1 μg/kg over 10 minutes followed by infusion 0.1–0.6 μg/kg/h during brachial plexus block for patients undergoing hand surgery is effective and safe method allowing to keep adequate haemodynamics and spontaneous breathing.
References
- Absalom, A. R., & Struys, M. Overview of Target Controlled Infusions and Total Intravenous Anaesthesia. Gent: Academia nPress, 2007.
- Arain, S. R., Ebert, T. J. The efficacy, side effects and recovery characteristics of dexmedetomidine versus propofol when used for intraoperative sedation. Anesthesia & Analgesia. 2002, 95: 461–466.
- Bhana, N., Goa, K. L., et al. Dexmedetomidine. Drugs. 2000. 59 (2): 263–268.
- Bienert, A., Wiczling, P. et al., Potential pitfalls of propofol target controlled infusion delivery related to its pharmacokinetics and pharmacodynamics. Pharmacological Reports. 2012, 64: 782–795.
- Brown, E., Solt, K., Purdon, P., Johnson-Akeju, O. Monitoring brain state during general anesthesia and sedation. In: Miller’s Anesthesia. 8th edition. London: Elsevier Health Sciences, 2014, 1: 1524–1530.
- Chan, W., Chang, S., Lin, C., Chen, M. & Fan, S. Target-controlled infusion of propofol versus intermittent bolus of a sedative cocktail regimen in deep sedation for gastrointestinal endoscopy: Comparison of cardiovascular and respiratory parameters. Journal of Digestive Diseases. 2013, 15 (1): 18–26.
- Choong, E., Loryan, I., Lindqvist, M., Nordling, Å, et al. Sex difference in formation of propofol metabolites: a replication study. Basic Clin Pharmacol Toxicol Basic & Clinical Pharmacology & Toxicology. 2013, 113 (2): 126–131.
- Cote, C. J., Wilson, S. Guidelines for monitoring and management of pediatric patients before, during, and after sedation for diagnostic and therapeutic procedures: Update 2016. Pediatrics. 2016, 138 (1): 1212.
- Dexmedetomidine description [online]. European Commision, Public Health. Brussels, Belgium – Available online: http://ec.europa.eu/health/documents/community-register/2013/20131218127652/anx_127652_lv.pdf (accessed on 20.03.2016).
- Ebert, T. J., Hall, J. E., Barney, J. A., Uhrich, T. D., et al. The effect of increasing plasma concentrations of dexmedetomidine in humans. Anesthesiology. 2000, 93: 382–394.
- Esmaoglu, A., Yegenoglu, F., Akin, A., Turk, C. Y. Dexmedetomidine added to levobupivacaine prolongs axillary brachial plexus block. Anesthesia & Analgesia. 2010, 111 (6): 1548–1551.
- Gertler, R., Brown, C., Mitchell, D. H., Silvius, E. N. Dexmedetomidine: a novel sedative-analgesic agent. Baylor University Medical Center Proceedings. 2001, 14: 13–21.
- Gotoda, T., Okada, H., Hori, K., Kawahara, Y., et al. Propofol sedation with a target-controlled infusion pump and bispectral index monitoring system in elderly patients during a complex upper endoscopy procedure. Gastrointestinal Endoscopy. 2016, 83 (4): 756–764.
- Grewal, A. Dexmedetomidine: new avenues. Journal of Anaesthesiology Clinical Pharmacology. 2011, 27 (3): 297–302.
- Gupta, P., Wellisch, O., Kronenfeld, M., Choueka, J., et al. Randomized trial of the use of dexmedetomidine vs. propofol after regional blockade in shoulder surgery patients in beach chair position. Open Journal of Anesthesiology. 2015. 05 (08): 187–191.
- Hawthorne, C., Sutcliffe, N. Total intravenous anaesthesia. Anaesthesia & Intensive Care Medicine. 2013, 14 (3): 129–131.
- Hohener, D., Blumenthal, S., Borgeat, A. Sedation and regional anaesthesia in the adult patient. British Journal of Anaesthesia. 2008, 100 (1): 8–16.
- Jiang, Y., Qiao, B., Wu, L., Lin, X. Application of narcotrend monitor for evaluation of depth of anesthesia in infants undergoing cardiac surgery: a prospective control study. Revista Brasileira de Anestesiologia. 2013, 63 (3); 273–278.
- Kaur, M., Singh, P. M. Current role of dexmedetomidine in clinical anesthesia and intensive care. Anesthesia: Essays and Researches. 2011, 5 (2): 128–133.
- Keating, G. M. Dexmedetomidine: a review of its use for sedation in the intensive care setting. Drugs. 2015. 75 (10): 1119–1130.
- Kilic, N., Sahin, S., Aksu, H., et al. Conscious sedation for endoscopic retrograde cholangiopancreatography: dexmedetomidine versus midazolam. The Eurasian Journal of Medicine. 2011, 43: 13–17.
- Ko, K., Jun, I., Lee, S., Lim, Y., et al. Effective dose of dexmedetomidine to induce adequate sedation in elderly patients under spinal anesthesia. Korean Journal of Anesthesiology Korean J Anesthesiol. 2015, 68 (6): 575.
- Kunisawa, T. Dexmedetomidine hydrochloride as a long-term sedative. Therapeutics and Clinical Risk Management. 2011, 7: 291–299.
- Ok, H. G., Baek, S. H., Baik, S. W., et al. Optimal dose of dexmedetomidine for sedation during spinal anesthesia. Korean Journal of Anesthesiology. 2013, 64 (5): 426–431.
- Paliwal, B. Comparison between dexmedetomidine and propofol with validation of bispectral index for sedation in mechanically ventilated intensive care patients. Journal of Clinical and Diagnostic Research. 2015.
- Sessler, C. N., Gosnell, M. S., Grap, M. J., et al. The Richmond agitation – sedation scale: validity and reliability in adult intensive care unit patients. American Journal of Respiratory and Critical Care Medicine. 2002, 166: 1338–1344.
- Shelly, M. P. Dexmedetomidine: a real innovation or more of the same? British Journal of Anaesthesia. 2001, 87 (5): 677–678.
- Song, J., Kim, W. M., Lee, S. H., Yoon, M. H. Dexmedetomidine for sedation of patients undergoing elective surgery under regional anesthesia. Korean Journal of Anesthesiology. 2013, 65 (3): 203–208.
- Stawicki, S. P. Sedation scales: very useful, very underused. OPUS 12 Scientist. 2007, 1 (2): 10–12.
- Venn, R. M., Hell, J., Grounds, R. M. Respiratory effects of dexmedetomidine in the surgical patient requiring intensive care. Critical Care. 2000, 4: 302–308.
- Venn, R. M., Karol, M. D., Grounds, R. M. Pharmacokinetics of dexmedetomidine infusions for sedation of postoperative patients requiring intensive care. British Journal of Anaesthesia. 2002, 88 (5): 669–675.
- Wang, T., Ge, S., Xiong, W., et al. Effects of different loading doses of dexmedetomidine on bispectral index under stepwise propofol target-controlled infusion. Pharmacology. 2013, 91: 1–6.
- Zhang, X., Bai, X. New therapeutic uses for an alpha2 adrenergic receptor agonist – dexmedetomidine in pain management. Neuroscience Letters. 2014, 561: 7–12.



