Influence of Noise in Ambulance Vehicles on Emergency Service Personnel in North Germany and Latvia
Abstract
Continuous noise exposure has an enormous damaging impact on hearing and general health status of the population. Although preventable, noise induced hearing loss (NIHL) is one of the most widespread irreversible occupational diseases worldwide, and thus is declared as a serious occupational hazard (World Health Organisation, 1997).
Several studies give evidence that noise creates physical and psychological stress, commonly presented as reduced attentiveness, sleep disturbances, cardiovascular dysfunction and mental health alteration (Jansen, 1967; OSHA, 2011).
Protection of health and from hazards at work should be in everybody’s interest. Therefore, the research aims for the evaluation of the impact of occupational noise on hearing, general security of health, quality of life and productivity of those working in stressful environments, which is shown in this study at the example of emergency service working personnel.
Introduction
Daily, noise has a ubiquitous potential hazardous effect on our body. The World Health Organisation (WHO) stated that worldwide 16 % of hearing loss in adults is attributed to occupational noise. NIHL is a sensorineural hearing loss, explained by permanent threshold shift of hearing sensitivity. NIHL not only affects the auditory system but also has psychosocial effects and is proved to have interference with general health by sleep disturbances or cardiovascular symptoms.
Aim
The aim of the study was to detect and define sound pressure levels that ambulance service workers are exposed to during their shifts in ambulance vehicle in North Germany and Latvia, especially with the focus on differences during signal and non-signal uses and different speed levels, and by this determine whether the noise has a hazardous character. Furthermore, the assessment of prevalence of auditory symptoms of the investigated personnel and possible correlations explaining NIHL are targeted, and finally the suggestion of protective measures to avoid further harm is proposed.
Methods
The collection of the study data is composed of two parts.
Firstly, the noise level in the ambulance vehicle was identified by measuring with the help of a Sound Level Meter (Model: Lutron SL-4013), which was placed at the level of the head of personnel in the front cabin of the ambulance vehicle. This equipment was programmed to collect data in fast mode, using the weighting curve “A”. Also protective foam in the microphone, in order to minimise other noise effects, was used. The ambulance cars were analysed in terms of technical specifications, physical dimensions for proper comparison of ambulance service in Germany and Latvia. For each country, four similar cars were chosen: Mercedes-Benz, Sprinter 315, CDI model, 4-door, manual, manufacturing year 2010/2014 (Riga, Latvia) and a similar model from year 2012 (Aurich, Germany) This model is a standard Sprinter with high ceilings. The front cabin design layout is constituted likewise.
The sirens are located bilaterally on the roof and front spoiler of the ambulance car.
The type of sirens and frequency for Latvia and Germany differ especially in frequency of sound melody. Germany uses sirens of type “Martin-Horn 2298 GM” DIN 14610 EC with a 4 membrane-bell and volume of 125 dB (A) at a one-metre distance.
Differences are found in frequency of sound melody. Due to road traffic regulations in Germany “§ 55 Abs. 3 S. 1 StVZO”, the following sound melody is mandatory for emergency vehicles “a’a’/d’d”. There is no standardised sound melody throughout a signal trip in Latvia, instead the driver can choose manually between different frequencies.
Measurements were recorded by the medical personnel during 20 emergency trips with a duration range from 10 to 15 minutes. These measurements were performed on different days, periods and shifts. During the constant speed of 50 km/h, 70 km/h and 100 km/h, the noise level was recorded carefully under equal conditions of weather, street condition, density of surrounded houses and closed windows and no radio.
The second part includes a questionnaire constituted of 14 questions sent electronically by the use of www.visidati.lv and distribution of printed format. In total n = 207 workers responded (Germany n = 102; Latvia, n = 105). The obtained data were analysed statistically by the use of SPSS 2013. For evaluation of relations between the groups, 2×2 Table Crosstabs and Pearson’s Chi-Square contingency test were used. Mann-Whitney test was used to detect frequencies among the survey population.
Results
In Germany the minimum noise level is measured at 50 km/h without signal use with 63.57 dB (A), and the maximum is measured at 100 km/h with signal use with 84.83 dB (A).
In comparison, in Latvia the minimum is measured at 50 km/h without signal use with 67.33 dB (A), and the maximum is measured at 100 km/h with signal use with 90.7 dB (A).
For both countries, it is noticeable that the noise level during signal use is enormously elevated compared to trips without signal use. Comparing Latvian with German emergency cars, non-signal trips are measured with a higher average noise level with a mean difference of 5.24 dB (A), and during signal use the noise level in Latvian emergency cars is also higher by an average difference of 2.47 dB (A). This means, Latvian emergency personnel is exposed to an overall higher noise level during emergency trips than German emergency personnel (see Table 1).
Comparing the two populations, Latvian emergency personnel is dominated by females whereas in Germany the majority is formed by men. Further, it is obvious that the Latvian emergency personnel in generally composed of a rather young team, age range of 18 to 30 years. In return, German personnel shows a wider range of age distribution, observed to be between 18 and 40 years; the vast majority of Latvian workers have been on average employed for five years, while the investigated German ambulance service personnel has been working on average over a 5-year period.
According to the amount of shifts per week and the density of emergency occurrence, both countries have four shifts of 12 hours during a seven day working week, and parallels are seen in the average amount of trips which are set at approximately six non-signal and five signal trips for both countries.
Evaluating the amount of hours the workers are exposed to noise during trips, the German ambulance service personnel is approximately 63 minutes longer exposed to noises from signal and 43 minutes longer exposed to non-signal noises during a 12-hour shift. Comparing both countries for their total emergency trip related noise exposure during a 12-hour shift, German personnel is in total exposed to noise 68 % of their work time, and Latvian personnel – 53 % in total (see Figure 1).
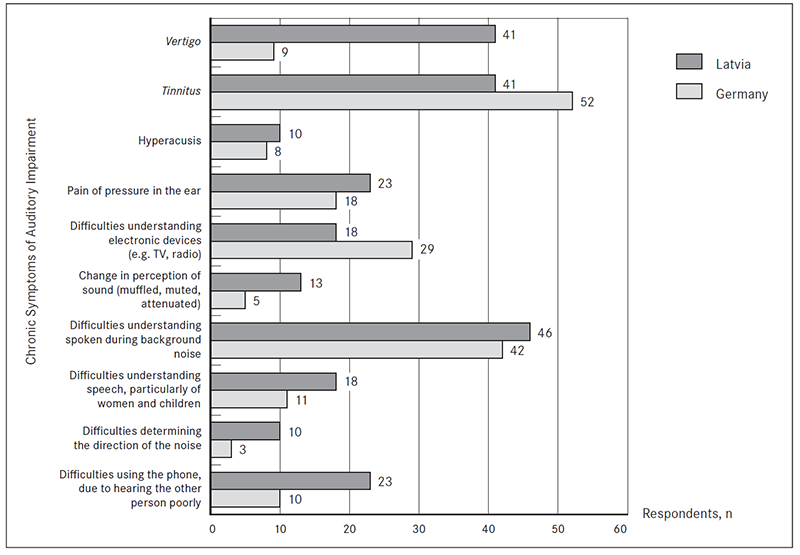
Looking closer at the NIHL symptoms given in the questionnaire, the respondents were allowed to choose more than one symptom, and indeed, most respondents indicated more than one symptom. Where, in comparison, Germans assigned 1–2 fitting symptoms and Latvians choose 2–3.
For both countries a common pattern of complaints and also highest incidences are found in the following two symptoms: difficulties of understanding during background noises (Germany 30.2 %, n = 42 and Latvia 26.6 %, n = 46) and tinnitus (Germany 38.8 %, n = 52 and Latvia 23.8 %, n = 41).
Other similarities but with lower frequency are given for hyperacusis (Germany 6 %, n = 6 and Latvia 5.8 %, n = 10), pain or pressure in the ear (Germany 13.4 %, n = 13.4 and Latvia 13.4 %, n = 23) and difficulties understanding speech, particularly women and children (Germany 7.9 %, n = 11 and Latvia 10.4 %, n = 18).
Comparing the main differences, Latvian emergency workers show a much higher incidence of symptoms such as vertigo (23.8 %, n = 41), changes in sound perception (7.5 %, n = 13), difficulties in determination of sound direction (5.8 %, n = 10) and difficulties using the phone due to poor understanding of the partner (13.3 %, n = 23).
German emergency personnel shows higher prevalence only for difficulties understanding electronic audio devices such as TV, radio thus need to increase the volume (20.9 %, n = 28) (see Figure 2).
Table 1. Results of noise level measured in dB (A) shown in total average and average of three different speed levels, Germany and Latvia in comparison
| Speed levels | Germany | Latvia | ||
|---|---|---|---|---|
| Without signal | With signal | Without signal | With signal | |
| Average | 66.6 | 84.8 | 71.9 | 86.6 |
| 50 km/h | 63.6 | 84.4 | 67.2 | 83.3 |
| 70 km/h | 65.2 | 84.8 | 72.4 | 85.9 |
| 100 km/h | 71.4 | 84.8 | 76.1 | 90.7 |
Figure 1. Time of exposure of the survey population to signal and non-signal trips during a 12-hour shift

* Others include the time during the 12-hour shift outside emergency car.
Figure 2. Prevalence of chronic auditory symptoms for each country of the survey population in absolute number, Germany and Latvia in comparison
Discussion
When persons with normal hearing are exposed to high noise levels over a prolonged period of time and by this reaching or exceeding the limit of permissible noise level exposure equivalent of 85 dB (A) over an 8-hour period, a shift of hearing threshold may appear. A threshold shift is an average deterioration of hearing 10 dB (A) or more in the frequency ranges of 2.000, 3.000 and 4.000 Hz in both ears, defined by Occupational Safety and Health Administration (OSHA, 2011).
This deterioration of hearing can be of a temporary nature, or, in opposite, at continuous exposition can result in a permanent threshold shift and hearing loss. The degree of hearing loss depends on the level of the sound pressure level, the duration of exposure, the frequency of noise and individual predispositions.
Applying this to the investigated population of the German and Latvian ambulance service, the Latvian personnel is exposed up to 5.24 dB (A) (non-signal) and 2.47 dB (A) (with signal) louder noise. Both countries demonstrate an exposure to hazardous noise level of approximately 85 dB (A) to 90 dB (A) during signal trips, which reaches and partly exceeds the exposure limits of 85 dB (A).
Sound measurements of this study show that during non-signal trips, the noise pressure level varies depending on the speed by 2–6 dB (A). The faster the speed level, the greater the noise level. During signal trips, Latvians experience and increase in noise level by 2–4 dB (A) depending on the speed level, but for Germans the noise level stays almost constant at different speed levels.
However, during a 12-hour shift, the Latvian survey population is exposed for approximately two hours to signal trips with an average noise level of approximately 87 dB (A), and the German survey population – approximately three hours to signal trips with an average noise level of 85 dB (A).
Referring to OSHA regulations, both countries are not exceeding the limit of permissible noise level exposure equivalent. Thus, the exposure to noise during emergency trips with signal are considered to be safe for the auditory system. Nonetheless, especially the Latvian emergency personnel indicates a great dominance for auditory changes, clearly shown in the study data. This indicates a failure of guidelines and imply a continuation of the study or re-evaluation of the guidelines.
Conclusion
Latvian emergency personnel clearly dominates with higher total number in eight out of ten auditory symptoms.
Statistical investigations for relations according to the study show that there is no significant relation between countries, age, gender or length of employment towards symptoms (p > 0.05) and thus cannot be attributed to the general population.
However, in a long-term view it is of importance to develop further preventive health measures for ambulance personnel in both countries, since the high noise levels during signal trips have harmful potential to the auditory system, health and subsequently, quality of life.
- NIHL is one of the oldest and most common occupational induced health issues worldwide.
- Common pattern and highest prevalence for auditory symptoms for both, Latvian and German ambulance services are:
- difficulties of understanding during background noises;
- tinnitus;
- vertigo;
- difficulties understanding electronic audio devices such as TV, radio, thus need to increase the volume.
- Latvian ambulance service personnel has a higher risk of development of NIHL due to high frequency of sound melody of the sirens and exposure to higher sound level during signal trips, caused by poor street conditions.
- For both countries, the noise level is remarkably elevated during signal trips compared to nonsignal trips.
- Speed level influences the noise level during trips without signal by 2–6 dB (A). The higher the speed, the higher the noise level during non-signal trips.
- During emergency trips with signal use, the noise level reaches and partly exceeds safety limits of 80–85 dB (A).
- Education of ambulance workers and management about preventive measures, importance of NIHL development and risk as well as regular audiometry check-ups are needed.
References
- World Health Organisation. 1997. Prevention of noise-induced hearing loss: Report of a WHO-PDH informal consultation. Geneva. Available from: http://apps.who.int/iris/bitstream/10665/65390/1/WHO_PDH_98.5.pdf (viewed 24.01.2018).
- OSHA (Occupational Safety and Health Administration). 2011. OSHA Technical Manual. [Online]. Available from: https://www.osha.gov/dts/osta/otm/new_noise/index.html#hearingloss [viewed 21.09.2016].
- Jansen, G. 1967. Zur Nervösen Belastung Durch Lärm (Eng. The nervous burden of noise). Berlin, Heidelberg: Springer- Verlag.


